
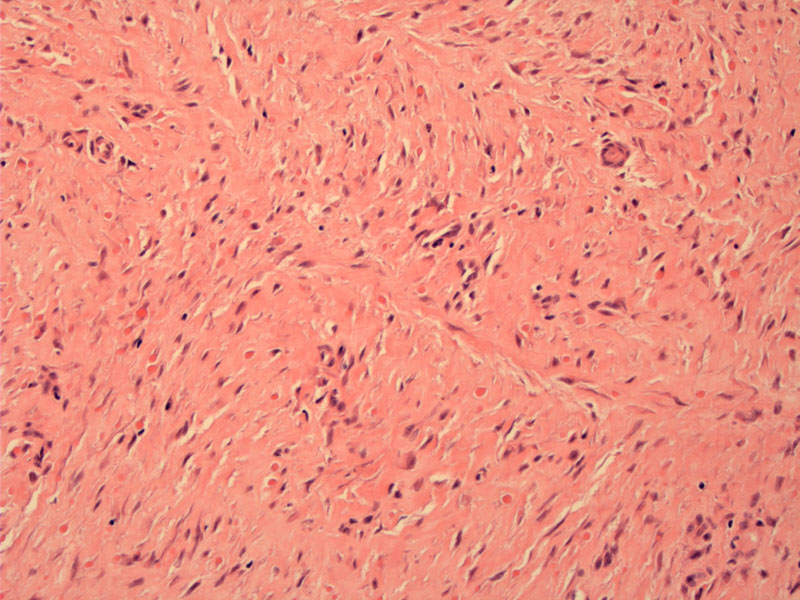
Inclusion body fibromatosis consists of a poorly circumscribed nodule located in the dermis with infiltration into adnexal structures. This dermal proliferation may lift the overlying epidermis, thus, form a protuberant polypoid nodule seen grossly and at low power. The overall picture is that of moderate cellularity. There is a proliferation bland spindled cells with elongated nuclei and pale eosinophilic cytoplasm which blends imperceptibly with a collagenous stroma.
){kind=link}
The hallmark feature is the presence of round eosinophilic intracytoplasmic inclusions found within the fibroblasts. A clear zone can be seen around the inclusions. This particular case shows many inclusions, but the number can vary from case to case. It is suggested that the inclusion bodies are composed of microfilaments of actin. Masson's Trichome would highlight the inclusion in bright red.
){kind=link}
Inclusion body fibromatosis, also known as infantile digital fibromatosis, arise almost exclusively in infants. They present as singular nodules (mean size 1 cm) in the lateral or dorsal surface of the distal digits. Oddly, the thumb and big toe are usually spared. One-third are present at time of birth, and the vast majority are solitary nodules, although a minority of cases have multiple or metachronous nodules.1,2
Because these lesions can and do present in adults, the name has been changed from infantile digital fibromatosis to inclusion body fibromatosis. Note that inclusion bodies, although pathognomonic for this entity, can vary in number from few to numerous; they are not present in every case.
A recent study conducted by Laskin demonstrated that the spindled cells comprising this tumor stain positively with calponin, desmin, smooth muscle actin, CD99 and CD117. However, the most useful stains to distinguish between inclusion body fibromatosis and other entites on the differential such as juvenile/infantile fibromatosis (desmoid-type), calcifying aponeurotic fibroma and infantile lipofibromatosis would be desmin.1
Inclusion body fibromatosis demonstrates strong diffuse desmin staining versus only focal staining in juvenile/infantile fibromatosis and completely absent staining in calcifying aponeurotic fibroma and infantile lipofibromatosis. Beta-catenin may be helpful in differentiating between inclusion body fibromatosis and desmoid-type fibromatosis, with the former demonstrating only very focal nuclear expression, and the latter with strong diffuse nuclear expression.1
Arises almost exclusively in infants of either sex. Usually small (less than 2cm) dome-shaped firm nodule located at the lateral surface of the 2nd to 4th digits. The vast majority are solitary.1
Biopsy is often required to confirm the diagnosis. Recurrence after excision is very common with reported rates of 61-75%.1 However, since these lesions may spontaneously regress, it has been recommended that the approach is to watch and wait after initial biopsy. Surgical excision should be considered for those with functional impairment or rapid growth.3
Benign entity with excellent prognosis.
1 Laskin WB, Miettinen M, Fetsch JF. Infantile digital fibroma/fibromatosis: a clinicopathologic and immunohistochemical study of 69 tumors from 57 patients with long-term follow-up. Am J Surg Pathol. 2009 Jan;33(1):1-13.
2 Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 1547.
3 Grenier N, Liang C, Capaldi L, Ney A, Lapidus C, Schappell D, Katarincic J, Robinson-Bostom L. Pediatr Dermatol. A range of histologic findings in infantile digital fibromatosis.2008 Jan-Feb;25(1):72-5.