
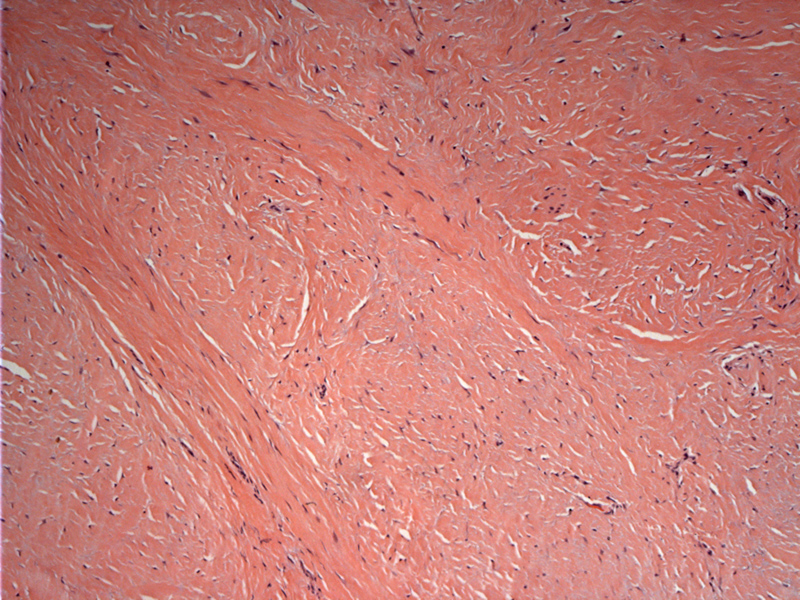
Hypocellular collagenous bands form the plaque. Although not seen here, aggregates of chronic inflammatory cells and secondary ossification are common features.
){kind=link}
The sclerotic tissue can be seen underlying the epidermis (top image).
){kind=link}
Penile fibromatosis, also known as Peyronie's disease, has been grouped together with palmar and plantar fibromatosis, however, these lesions are probably unrelated (Fletcher). However, a subset of patients do present with both Peyronie's disease and palmar fibromatoses.
Histologically, there is a hypocellular, variably hyalinzed collagenous plaque. Clusters of chronic inflammatory cells and metaplastic ossification within the scar are common features.
Mostly affects men between ages 40-60. A history of penile trauma and urethritis is present in some instances, suggesting a sclerosing inflammatory process in the genesis of the lesion (Jalkut, Rosai).
It presents as an indurated plaque or indentation in the corpora cavernosa, leading to deformation and curvatuve of the penis upon erection. 30% of cases are associated with erectile dysfunction, which is likely multifactorial e.g. vascular compromise, anxiety.
Initial management is conservation and includes systemic therapy (colchicine which inhibits collagen synthesis), topical therapy and intralesional injections. For those who fail medical management, surgery can be an option (Jalkut).
Benign condition without systemic sequelae.
• Fibrous : Palmar Fibromatosis
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 1551.
Jalkut M, Gonzalez-Cadavid N, Rajfer J. Peyronie's Disease: A Review. Rev Urol. 2003 Summer;5(3):142-8.
Rosai, J. Rosai and Ackerman's Surgical Pathology. 9th Ed. Philadelphia, PA: Elsevier; 2004: 1467-8.