
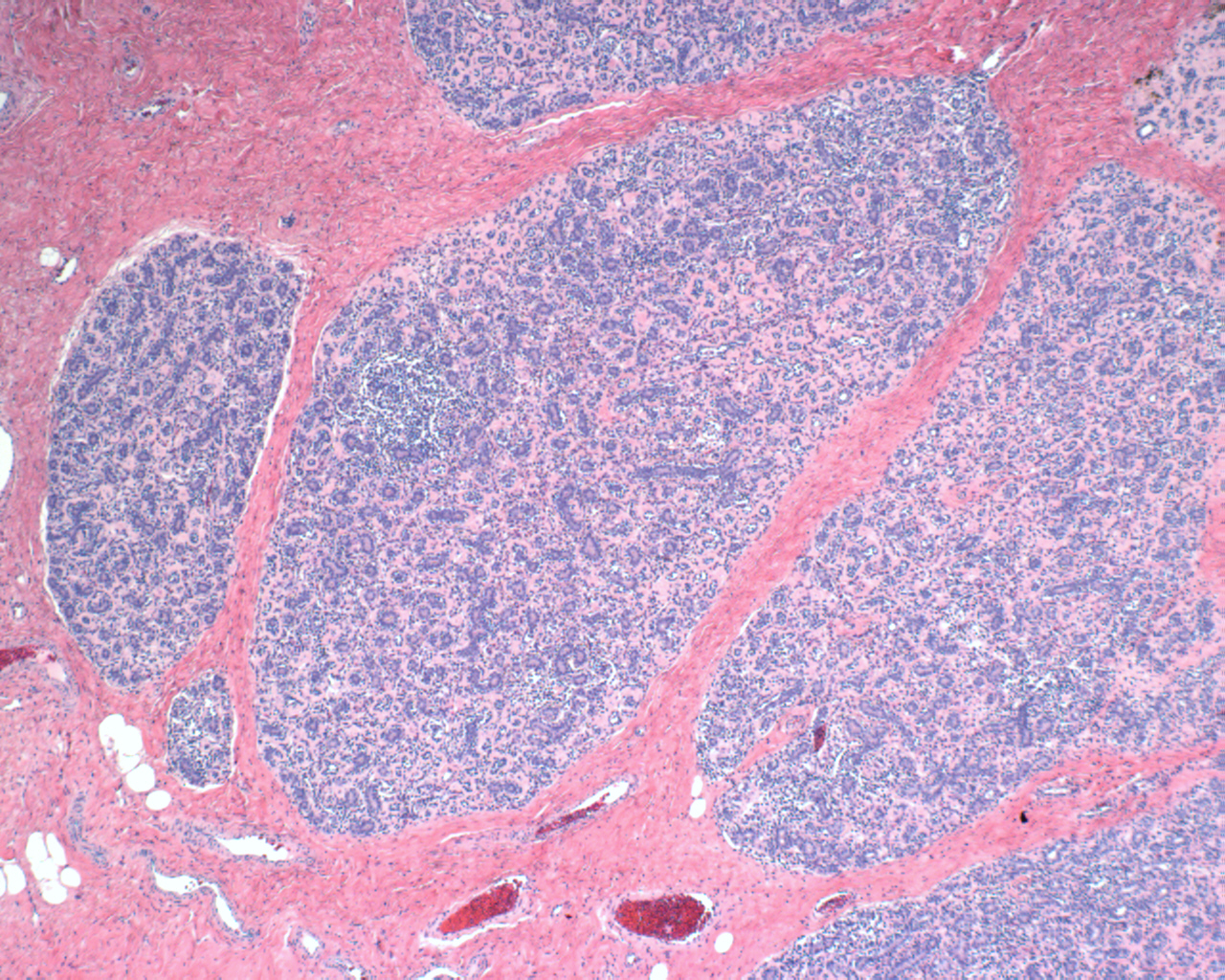
Case 1: Well-circumscribed lobules of myoepithelial cells and epithelial cells embedded in a fairly dense stroma.
Tubules are formed by two cell components -- myoepithelial cells with clear cytoplasm underlying the darker epithelial cells. Some cases may have a papillary architecture.
Case 2: As is typical for this lesion, it appears fairly well circumscribed but unencapsulated. The myoepithelial cells grow in a more spindled pattern whereas in case 1, the myoepithelial proliferation is more lobular.
A proliferation of myoepithelial cells (some appearing spindled) surround variably sized and shaped tubules. Some cases may have sebaceous or even myxochondroid differentation (not seen here).
Myoepithelial lesions of the breast can be divided into myoepitheliosis, adenomyoepithelioma and malignant myoepithelioma (myoepithelial carcinoma), with the latter composed solely of myoepithelial cells and the former two entities composed of myoepithelial cells and epithelial cells.
Adenomyoepithelioma is a biphasic well-circumscribed tumor consisting of proliferation myoepithelial cells surrounding benign epithelial-lined spaces. These lesions are often circumscribed and quite firm, but they may also be soft or have ill-defined margins, and occasionally contain small cysts.
Histologically, tubular or glandular structures (epithelial-lined spaces) are surrounded by myoepithelial cells, which are usually polygonal with clear cytoplasm, but may be spindled. The expansive myoepithelial component can be evenly distributed or nested/nodular (Kempson). Pink basement membrane material elaborated by the myoepithelial cells may stream between the tubules.
Adenomyoepitheliomas can be classified as spindle-cell, tubular and lobulated depending on their growth patterns. A similar tumor (epithelial-myoepithelial carcinoma) arises from myoepithelial cells in the salivary gland (Howlett).
Cytokeratins (e.g. CAM5.2, CK7 or AE1/3) will highlight the epithelial component while the myoepithelial component will stain with S100, SMA (variable staining), muscle specific actin, calponin and desmin (McLaren).
Rare lesion that present as a palpable nontender mass. Rapid enlargement is suggestive of malignant transformation.
Excision with clear margins is recommended.
Most are benign, but rare cases of recurrence or malignant transformation have been described. The propensity for satellite nodules is thought to account for at least some of the cases of local recurrence. Aggressive features include irregular margins, a high mitotic count (>11-14 MF per 10 HPF), cytologically malignant myoepithelial cells and a solid growth pattern (Loose, Kihara). Malignant transformation (of either or both elements) has a significant likelihood of both local recurrence and metastases, particularly to the lung and brain (Tavassoli, Loose).
While some authors suggest that these tumors be called malignant adenomyoepitheliomas, McLaren and colleagues (2005) recommends that the term adenomyoepithelioma should be discarded in such instances and instead, the tumor should be designated as a carcinoma, sarcoma or myoepithelial carcinoma to emphasize its malignant nature.
→ Biphasic tumor with a proliferation of epithelial and myoepithelial components.
→ Although easily recognized in an excised specimen, these lesions can be difficult to diagnose on core biopsy.
Howlett DC et al. Adenomyoepithelioma of the Breast: Spectrum of Disease with Associated Imaging and Pathology. AJR 2003;180:799-803.
Kihara M et al. Malignant adenomyoepithelioma of the breast with lung metastases: report of a case. Surg Today. 2001;31(10):899-903.
Loose JH et al. Adenomyoepithelioma of the breast. A spectrum of biologic behavior. Am J Surg Pathol. 1992 Sep;16(9):868-76.
McLaren BK, et al. Adenomyoepithelioma: clinical, histologic, and immunohistologic evaluation of a series of related lesions. Am J Surg Pathol. 2005 Oct;29(10):1294-9.
Tavassoli FA. Myoepithelial lesions of the breast. Myoepitheliosis, adenomyoepithelioma, and myoepithelial carcinoma. Am J Surg Pathol. 1991 Jun;15(6):554-68.

){kind=link}
){kind=link}
){kind=link}
){kind=link}