
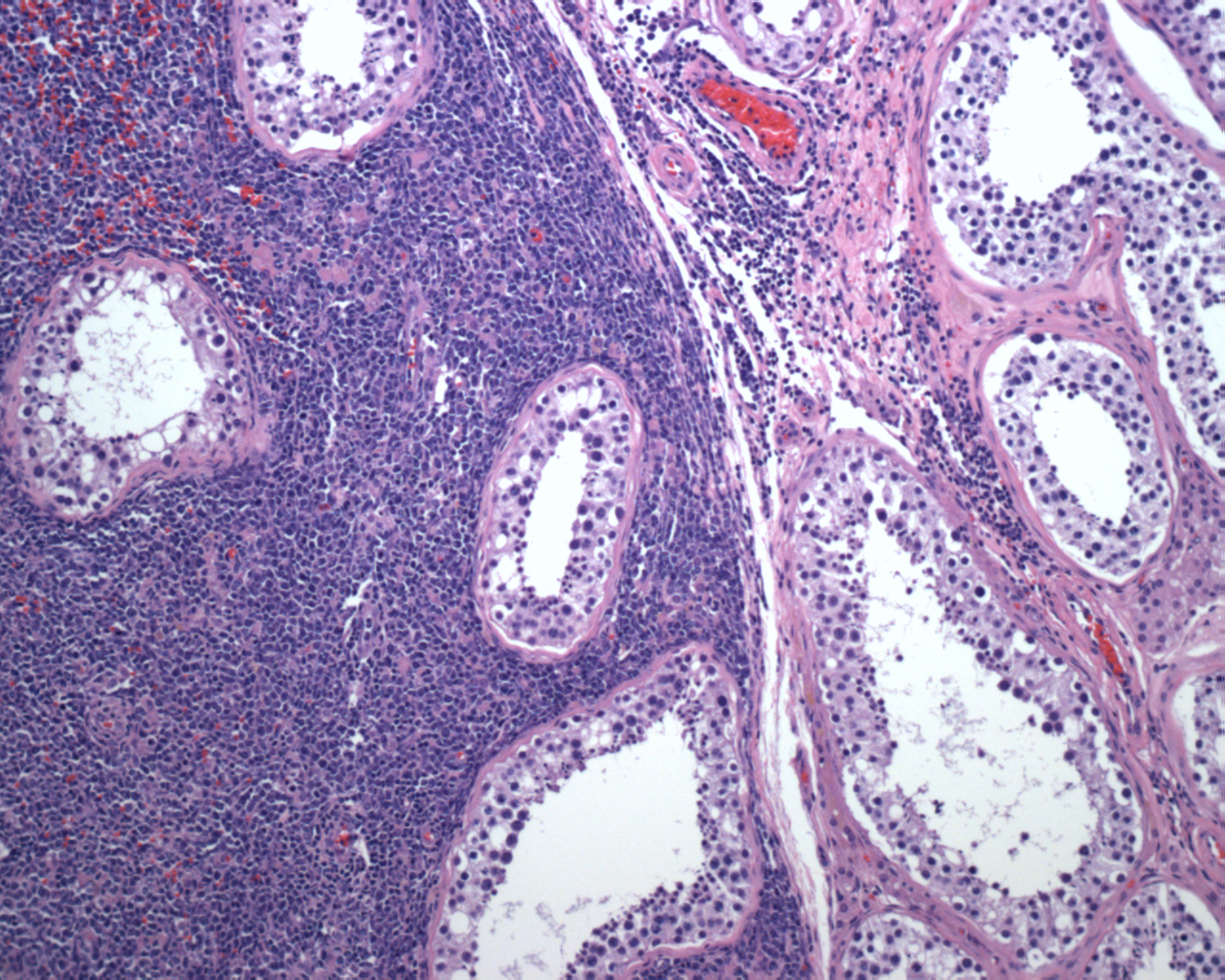
One can appreciate the junction between normal seminiferous tubules (right) and those involved by neoplastic lymphoma cells (left). The neoplasm is characterized by sheets and cords of malignant lymphocytes, infiltrate the interstitum and surround the seminiferous tubules. Cytologic atypia, mitotic activity and necrosis are prominent.
){kind=link}
A higher power image of the lymphoma cells shows how they do not destroy but they surround the seminiferous tubule.
){kind=link}
A high Ki67 suggests a more aggressive tumor and is a poor prognostic factor.
){kind=link}
BCL-2 is positive.
){kind=link}
BCL-6 is weak and focal, would be expected in the non-germinal center like subtype.
){kind=link}
CD10 is negative.
){kind=link}
As expected, CD20 is strongly positive, corroborating the B-cell immunophenotype.
){kind=link}
Primary testicular lymphoma comprises approximately 5% of all testicular neoplasms, however, it is the most common malignant tumor in men older than 50. Diffuse large B-cell lymphoma is the most common subtype (80-90% of cases), and the remainder are marginal zone lymphoma, follicular lymphoma, anaplastic large cell lymphoma and T-cell lymphoma. Note that in a young child, testicular lymphoma is mostly due to the secondary involvement by Burkitt lymphoma or lymphoblastic lymphoma.
The neoplastic cells are positive for CD20, CD45, Bcl2 and negative for Bcl6, CD10, CD3, CD117, PLAP, and OCT3/4. Note that CD117, PLAP and OCT3/4 would be positive in seminomas. This profile is consistent with the non-germinal center like DLBCL (CD10-, Bcl6-, MUM1+) which carries a worse prognosis and comprises ~90% of cases. The non-GC types also are strongly Bcl2 positive and have a high proliferative rate as demonstrated by Ki-67 >40-50% (Horne, Al-Abbadi).
The germinal-center like variant has a different IHC profile (CD10+ and/or Bcl6+ and MUM1-), and carries a more favorable prognosis. ~10% of DLBCL of testis belongs to this group.
The differential diagnosis includes seminoma (distinct cell membranes, squared nuclear contours, seminiferous tubules are involved versus spared in lymphoma, positive for PLAP, OCT3/4, D240 and CD117), embryonal carcinoma (epithelial appearances, vesicular nuclei, ITGCN, positive for PLAP, OCT3/4, CK and CD30, negative for lymphoid markers as well as D240 and CD117). Chronic orchitis may also enter the differential with a inflammatory infiltrate surrounding tubules, however, the infiltrate is benign, mixed and often granulomatous, not clonal like DLBCL.
Testicular lymphoma is the most common testicular neoplasm in men over 50. Usually presents is unilateral painless swelling of the testicle. Systemic symptoms (fever, anoxeria, night sweats) may be present in a subset of patients. Serum LDH may be useful in assessing tumor bulk as well as response to therapy (Horne).
Prognosis is poor. Regional spread to retroperitoneal lymph nodes often develops. Relapse occurs in >50% of cases. In relapses, non-contiguous extra-nodal sites are involved, usually the contralateral testis, CNS and Waldeyer's ring (the lymphoid tissue ring located in the pharynx). Involvement of the latter two structures is ominous. The skin, lung, pleura and soft tissues can also be affected (Horne).
Al-Abbadi MA, et al. Primary testicular diffuse large B-cell lymphoma belongs to the nongerminal center B-cell-like subgroup: A study of 18 cases. Mod Pathol. 2006 Dec;19(12):1521-7. Epub 2006 Sep 22.
Horne MJ, Adeniran AJ. Primary diffuse large B-cell lymphoma of the testis. Arch Pathol Lab Med. 2011 Oct;135(10):1363-7.