){kind=link}
Meningiomas account for approximately 28% of primary CNS tumors (Fletcher) and arise from arachnoid cap cells, which line the inner dura mater. Favored sites within the cranium include the falx, cerebral convexities, olfactory grooves, sphenoidal ridge, and suprasellar region (Fletcher). Arachnoid cells are found in the stroma of the choroid plexus, and thus, meningiomas can also arise in the ventricles; the left lateral ventricle is most common, followed by the third ventricle (Fletcher). The cerebellopontine angle is common location in the posterior fossa.
Grossly, meningiomas are dural-based well-circumscribed tan-yellow rubbery masses that compress underlying parenchyma. It is covered by fibrous tissue and may have a bosselated or polypoid surface. It may occasionally grow as a plaque (usually along the sphenoid ridge), spreading along the surface of the dura and elicit hyperostosis in the overlying calvarium (Kumar).
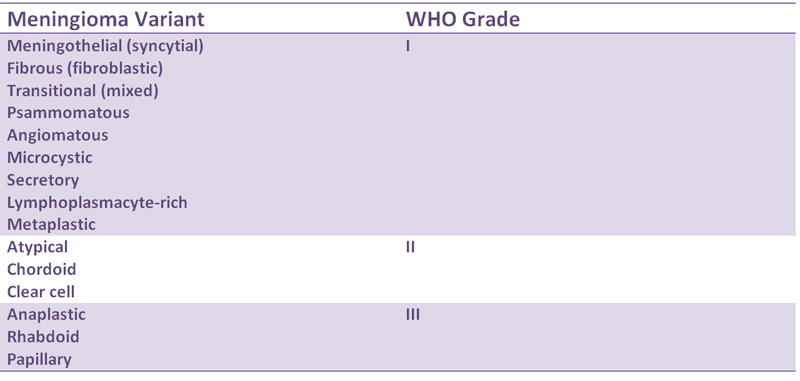
There is a large number of histologic variants including:
- Syncytial (Meningotheliomatous)
- Fibroblastic
- Transitional (mixed)
- Psammomatous
- Angiomatous
- Microcystic
- Secretory
- Lymphoplasmocyte-Rich
- Metaplastic
- Chordoid
- Clear Cell
Most meningiomas are of the syncytial, fibrous or transitional (combination of fibrous and syncytial) types. The nuceli are oval or round with inconspicuous nucleoli. Psammoma bodies are common and intranuclear pseudoinclusions (actually cytoplasmic invaginations) may be seen.
The most common molecular aberration is the loss of chromosome 22, especially 22q (long arm). Note that 22q12 contains the NF2 gene, and interestingly, 50% of mengingiomas not associated with NF2 harbor mutations in the NF2 gene (Kumar).
Due to the numerous histologic variants, the differential diagnosis is very broad. Most mengiomas are positive for vimentin, EMA (80%), S100 (20% to 40%) and GFAP negative (Prayson).
Usually a benign tumor seen in the adults and is rare in childhood. There is a female predominance (F:M ratio of 3:1), however, atypical and malignant meningomas are more common in males (Prayson). Epidural tumors are more common in children. These are usually slow growing lesions and symptoms depend on which are of the brain the tumor is compressing.
There is an association with NF2, in which case, multiple meningiomas may be seen. Patients with a history of previous radiation may also be more predisposed to developing meningiomas. Some meningiomas have PR receptors and rapid growth during pregnancy has been documented (Kumar).
Meningiomas and its variants are considered fairly indolent tumors (WHO Grade I). There is low risk of recurrence. Atypical meningiomas (WHO Grade II) and anaplastic meningiomas (WHO Grade III) are more aggressive tumors.
Recurrent rates in WHO Grade I tumors range from 7% to 20%; WHO Grade II tumors range from 29% to 40% and WHO Grade II tumors range from 50% to 78% (Prayson).
• Meninges : Meningioma, Transitional Variant
• Meninges : Atypical Meningioma
• Meninges : Meningioma, Anaplastic Variant
• Meninges : Meningioma, Angiomatous Variant
• Meninges : Meningioma, Chordoid Variant
• Meninges : Meningioma, Clear Cell Variant
• Meninges : Meningioma, Fibrous Variant
• Meninges : Meningioma, Meningotheliomatous (Syncytial) Variant
• Meninges : Meningioma, Microcystic Variant
• Meninges : Meningioma, Psammomatous Variant
• Meninges : Meningioma, Secretory Variant
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 1707-1710.
Kumar V, Abbas AK, Fausto N. Robbins and Cotran Pathologic Basis of Disease. 7th Ed. Philadelphia, PA: Elsevier; 2005: 1409-1410
Prayson, RA. Neuropathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elvesier; 2005: 489-494.