
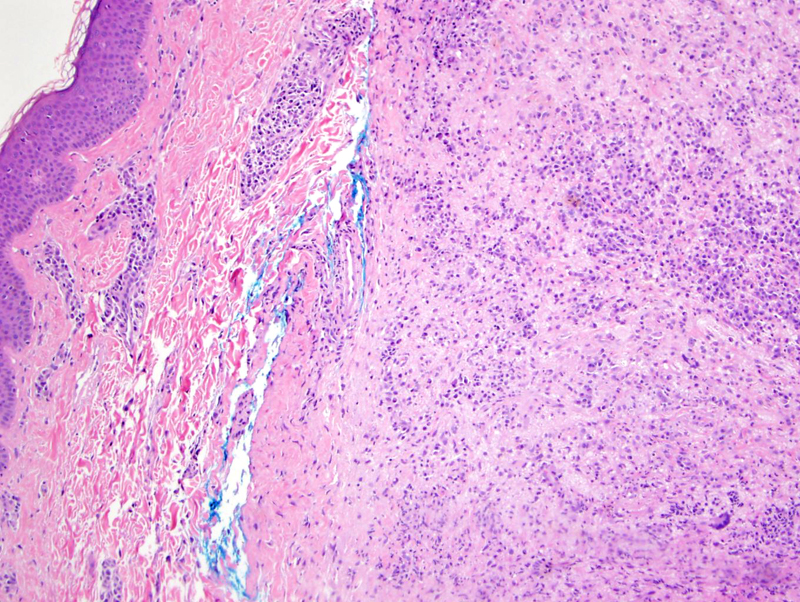
Dermal aggregates of pale pink foamy cells can be seen.
){kind=link}
Foamy histiocytes (SHML cells) with interspersed lymphocytes and plasma cells can be seen at higher power. Emperipolesis is not obvious in this image, but was present in the case.
){kind=link}
Rosai Dorfman Disease, a.k.a. sinus histiocytosis with massive lymphadenopathy (SHML), is a rare histiocytosis that presents classically as massive cervical lymphadenopathy in young children. Accompanying symptoms include fever, night sweats and weight loss. The pathogenesis is not fully understood and proposed theories include immune dysregulation and viral infections (e.g. EBV, HHV-6).
Extranodal involvement is seen in up to 40% of cases, with the most frequent sites being skin, soft tissue, upper respiratory tract, bone and eye. Head and neck involvement has been reported in 22% of cases, most commonly the nasal cavity followed by the parotid gland (Juskevicius). Other sites include the GI tract, GU tract, breast, lungs, liver and pancreas.
Note that extranodal SHML may not have nodal involvement. This is especially the case in cutaneous SHML and sinonasal SHML, where most cases are limited to the skin and sinonasal tract, respectively (Frater, Chen).
Similar to SHML elsewhere, the disease is typified by a proliferation of histiocytes accompanied by a mixed inflammatory infiltrate. Emperipolesis (histiocytes engulfing lymphocytes and rarely, plasma cells and neutrophils) is highly characteristic.
Of note, primary cutaneous SHML demonstrates a different clinical profile than systemic SHML in that cutaneous SHML tends to affect older, white female patients (Frater).
On clinical exam, cutanenous SHML presents as clusters of reddish papules. Laboratory abnormalities may include cytopenias and hypergammaglobulinemia (Frater, Van Zander).
Cutaneous Rosai-Dorfman disease has a benign course usually with spontaneous regression.
→Compared with patients with systemic SHML, those primary cutaneous disease have a different demographic profile: they are more likely to be older, female and white.
• Sinonasal : Rosai-Dorfman Disease
• Dermis : Cutaneous Rosai-Dorfman Disease
• Lymph Nodes : Rosai-Dorfman Disease
Chen HH, et al. Factors associated with recurrence and therapeutic strategies for sinonasal rosai-dorfman disease. Head Neck. 2011 Aug 4. doi: 10.1002/hed.21832. [Epub ahead of print]
Frater JL, et al. Cutaneous Rosai-Dorfman disease: comprehensive review of cases reported in the medical literature since 1990 and presentation of an illustrative case. J Cutan Med Surg. 2006 Nov-Dec;10(6):281-90.
Juskevicius R, and Finlay JL. Rosai-Dorfman disease of the parotid gland, cytologic and histopathologic findings with immunohistochemical correlation. Arch Pathol Lab Med 2001; 125: 1348-1350.
Van Zander J. Cutaneous Rosai-Dorfman disease. Dermatol Online J. 2004 Nov 30;10(3):12.