
Erythema nodosum is characterized by septal fibrosis and septal inflammation. The inflammatory infiltrate is mixed, composed of lymphocytes, histiocytes, neutrophils, eosinophils and multinucleated giant cells.
){kind=link}
The inflammation affects predominantly the septae between the fat lobules. The inflammation often extends from the septae into the periphery of the fat lobules.
){kind=link}
Collections of macrophages around small blood vessels or slitlike spaces known as Miescher's nodules or Miescher's radial granulomas are said to be fairly specific features of EN (Busam).
){kind=link}
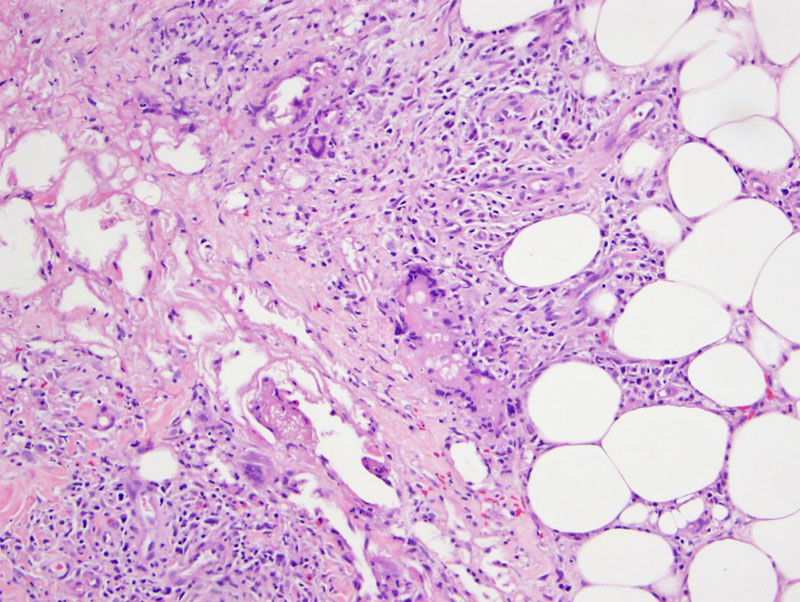
Giant cells cluster to form a nice granuloma with surrounding inflammation and some fibrosis.
){kind=link}
The quality of the inflammatory infiltrate in the septa varies with the age of the lesion. Early lesions consist of edema, hemorrhage, and neutrophils which later develop into fibrosis, periseptal granulation tissue, lymphocytes, and multinucleated giant cells later.
){kind=link}
Panniculitis is inflammation of the subcutaneous fat and it has historically been very difficult to classify. Most textbooks broadly categorize panniculitis as "septal" (inflammation involving primarily the septae coursing between the lobules of fat) or "lobular" (inflammation involving mainly the lobules of fat themselves).
However, this classification is problematic because other than erythema nodosum (purely septal inflammation), most other entities exhibit a mixture of septal and lobular inflammation. Furthermore, the histology will change depending on the stage of the disease (Rapini).
Erythema nodosum (EN) is the most common type of panniculitis, as mentioned previously, and is primarily a septal panniculitis.
Clinically, these present as red tender nodules, usually on the shins. Precipitating factors include infection (e.g. streptococcal infection, Yersinia, coccidioidomyosis), drugs (oral contraceptives, sulfonamides), sarcoidosis, malignancies (leukdemia, Hodgkin lymphoma), among many others.
→EN is a primarily septal panniculitis.
→Presents commonly as painful nodules of the shins, with OCPs and infections as common precipating factors.
→An inflammatory infiltrate composed of lymphocytes, histiocytes, neutrophils and eosinophils is larger confined to the septae, although it may spill over into the periphery of the lobules.
Busam KJ. Dermatopathology: Foundations in Diagnostic Pathology 1st Ed. Philadelphia, PA: Elsevier; 2010: 84-5.
Rapini RP. Practical Dermatopathology. Philadelphia, PA: Elsevier; 2005: 213-4.