
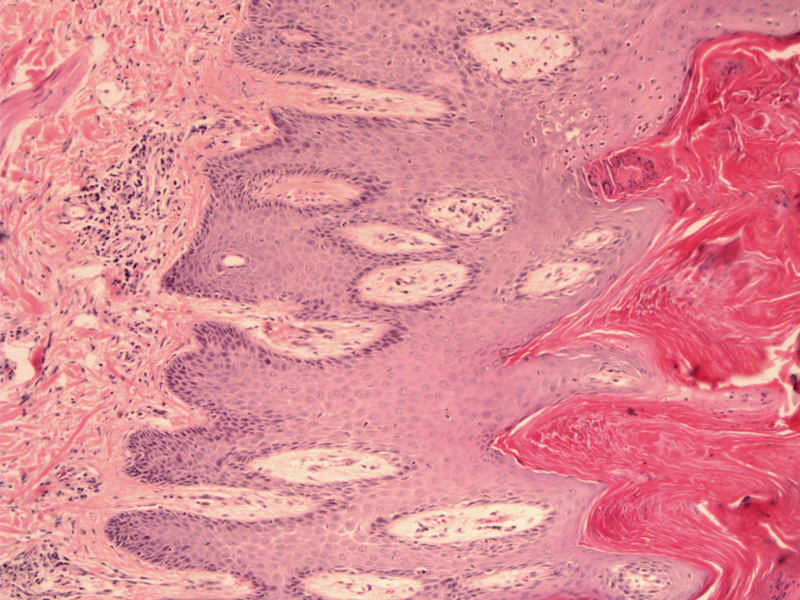
Case 1: Features of psoriasis demonstrated here include confluent parakeratosis, neutrophils in the stratum corneum, regular acanthosis, suprapapillary thinning of epidermis and hypogranulosis.
){kind=link}
Psoriasis is a familial disease that affects approximately 1-3% of the population. The cause is complex, with an interaction between environmental triggers and inheritance of susceptibility alleles. It is not due to allergy.
Psoriatic arthritis affects about 10% of patients and usually does not arise for about 10 years after the skin lesions.
Sharply demarcated plaques arise extensor surfaces of elbows and knees, the lumbosacral area, intergluteal cleft, and scalp, but any body site can be affected. In inverse psoriasis, lesions appear in intertriginous areas. It is uncommon on the face, as UV light improves the condition (Rapini).
The plaques are erythematous with loosely adherent,silvery-white scales. Removal of the scale can induce punctated leeding, referred to as the Auspitz sign.
Often, there are nail changes such as pitting. Psoriatic arthritis, an inflammatory, seronegative spondyloarthropathy, affects 1/3 of patients.
The vast majority have mild-to-moderate disease, most of which is treated with high dose topical steroids. Severe disease can be managed with methotrexate or ultraviolet light–based therapy.
→Features of psoriasis include confluent parakeratosis, regular acanthosis, suprapapillary thinning, absence of granular layer and Munro micrabsesses (collections of neutrophils within the parakeratotic scale).
Busam KJ. Dermatopathology: Foundations in Diagnostic Pathology 1st Ed. Philadelphia, PA: Elsevier; 2010: 21-5.
Rapini RP.Practical Dermatopathology. Philadelphia, PA: Elsevier; 2005: 51-3.