
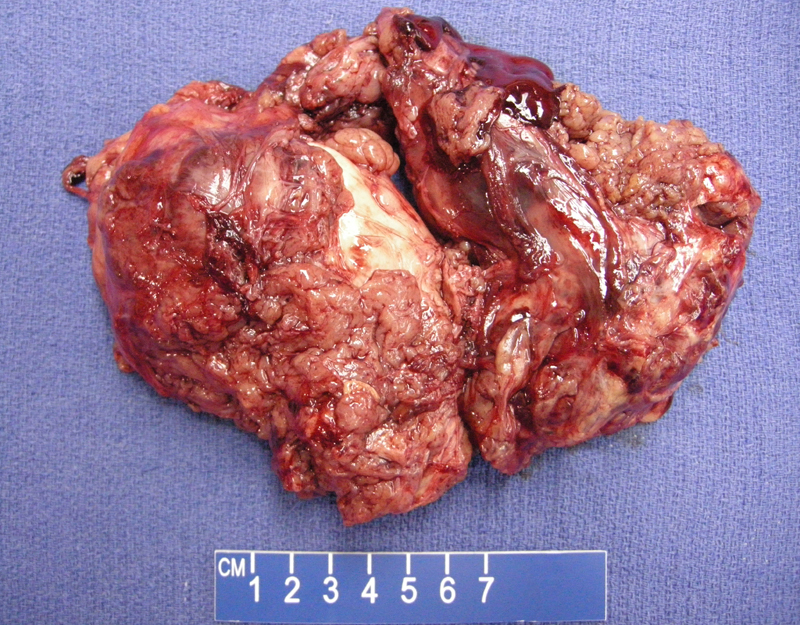
This is a 18 cm resection of lobulated firm tan-brown mass removed from the thigh. SFT can vary from 1 cm to up to 30 cm. Only about 5% of these tumors arise in the lower extremity.
){kind=link}
A hemangiopericytoma-like vascular pattern is easily identified.
){kind=link}
Mitotic activity (arrow) should not exceed 4 MF per 10 HPF. If this is the case, consider a malignant SFT. The cells are randomly arranged.
){kind=link}
A proliferation of spindled to oval cells is seen here. The cells show relative uniformity. Other key features of SFT such as a patternless pattern, keloid collagen and alternating zones of cellularity as not as well demonstrated here.
){kind=link}
Solitary fibrous tumor (formerly hemangiopericytoma) were thought to arise mainly from mesothelial surfaces (i.e. pleura), but it is now known that extrapleural lesions are more common than pleural ones. SFT can arise almost anywhere in the body including peritoneum, retroperitoneum, mediastinum, upper respiratory tract, orbit and soft tissues (Fletcher).
Grossly, the tumor is large and lobulated with a pale-tan, rubbery cut surface. Histologically, there is a "patternless" pattern, with proliferations of bland spindled/epithelioid cells in fascicles. Key features include alternations of hypercellular and hypocelluar regions, interspersed keloidal collagen bands and a prominent "hemangiopericytoma-like" branching vasculature.
Mitotic activity is spare and if greather than 4 MF per 10 HPF, a malignant SFT should be considered. SFT are CD34 and CD 99 positive and negative for S-100, actin, desmin and keratin. This immunohistochemcical profile is helpful in distinguishing SFT from other entities on the differential such as synovial sarcoma, malignant peripheral nerve sheath tumor, desmoplastic mesothelioma and so on (Fletcher, Folpe).
Occurs in adults and presents as a large-growing mass. Extra-pleural SFTs arise intra-abdominally but also in the head and neck, meningeal, orbit, and urogenital tract.
SFT can cause paraneoplastic syndromes such as hyperglycemia due to elaboration of an insulin-like growth fact and hypertrophic osteoarthropathy. Of note, hypertrophic osteoarthropathy is usually secondary to cardiac or pulmonary dysfunction such as bronchogenic carcinoma, right to left shunts, lung abscesses and intrathoracic neoplasms (Fridlington). Thus, digital clubbing is more often seen in large pleural-based SFT rather than extrapleural SFT.
Hypertrophic osteoarthropathy is a syndrome characterized by finger clubbing, hypertrophic skin changes, and periosteal bone changes.
Benign; but there is a clinical spectrum, as in 5-10% of cases, they behave aggressively with local recurrence and metastases.
- SFT can cause paraneoplastic syndromes such as hyperglycemia due to elaboration of an insulin-like growth fact and hypertrophic osteoarthropathy
-SFT is CD34 and CD 99 positive
• Sinonasal : Solitary Fibrous Tumor
• Pleura : Solitary Fibrous Tumor
• Uncertain Lineage : Hemangiopericytoma
• Uncertain Lineage : Synovial Sarcoma
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 1549-1550.
Folpe AL, Inwards CY. Bone and Soft Tissue Pathology: Foundations in Diagnostic Pathology Philadelphia, PA: Elsevier; 2010: 146-150.
Fridlington J, Weaver J, Kelly B, Kelly E. Secondary hypertrophic osteoarthropathy associated with solitary fibrous tumor of the lung. J Am Acad Dermatol. 2007 Nov;57(5 Suppl):S106-10.