
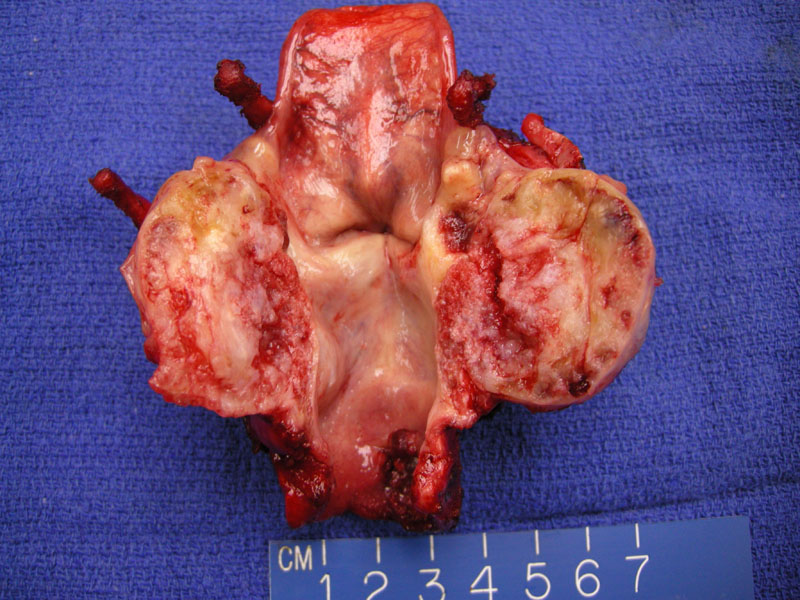
An expansile and infiltrative solid glistening mass is seen arising in the region of the cricoid. The histology is low grade.
){kind=link}
Grossly the origin from the cricoid cartilage is evident. This is the most common origin for laryngeal chondrosarcoma
){kind=link}
Irregular growth of the chondroid neoplasm into normal bone and skeletal muscle is apparent.
){kind=link}
A well-defined lobule of chondrosarcoma is seen here undermining the normal surface mucosa, which remained intact. This appearance is that of the chondrocytic chondrosarcoma subtype, by far the most common type.
){kind=link}
The neoplasm is low grade cytologically and by cellular criteria and grows in a lobulated fashion as low grade tumor are expected to do. The majority of such tumors in this site are either low grade or at most moderate.
){kind=link}
The vast majority of larygeal chondrosarcomas arise in older men and are low or moderate grade slow growing neoplasms. Tumors usually arise from the posterior lamina of the cricoid cartilage (78%) or thyroid cartilage (18%), and rarely from the arytenoids and epiglottis (Rinaldo). They generally causes local destruction due to a mass effect before invading surrounding tissues (Bathala).
Signs and symptoms relate to tumor location, with those arising cricoid cartilage
presenting with dyspnea, hoarseness and dysphagia, while cricoid tumors may cause vocal cord paralysis. Tumors arising from the thyroid cartilage may present as an asymptomatic neck
mass.
On CT scan, chondrosarcomas show fine, punctuate, stippled to coarse (‘popcorn’) calcifications (Wang).
Initially treated with voice-preserving conservative surgical excision, reserving more aggressive surgery for larger tumors or tumor recurrences.
Overall very good. This tumor often shows slow indolent growth but may locally recurrence (approximately 20%), with infrequent metastases (Thompson).
Bathala S, Berry S, Evans RA, Brodie S, Altaan O. Chondrosarcoma of larynx: review of literature and clinical experience. J Laryngol Otol. 2008 Oct;122(10):1127-9.
Rinaldo A, Howard DJ, Ferlito A. Laryngeal chondrosarcoma: a 24 year experience at Royal National Throat Nose and Ear Hospital. Acta Otolaryngol 2000;120:680–8
Wang SJ, Borges A, Lufkin RB, Se Carz JA, Wang MB. Chondroid tumours of larynx computed tomography
finding. Am J Otolaryngol 1999;206:379–82.
Thompson LD, Gannon FH. Chondrosarcoma of the larynx: a clinicopathologic study of 111 cases with a review of the literature. Am J Surg Pathol. 2002 Jul;26(7):836-51.