
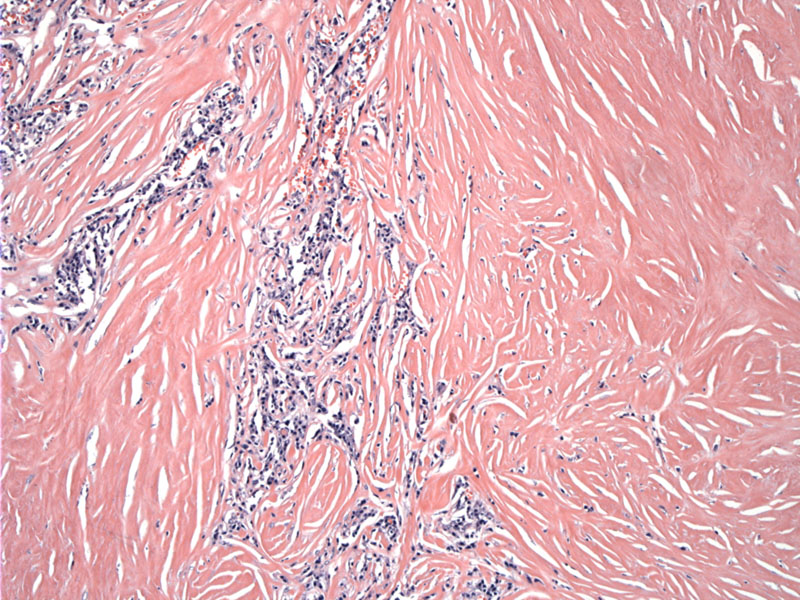
Dense bands of keloidal collagen replace large areas of thyroid parenchyma.
){kind=link}
The fibrotic bands compartmentalize the architecture.
){kind=link}
There is oncocytic change to the follicular epithelium.
){kind=link}
Sclerosis microcompartmentalizes the epithelium as well.
){kind=link}
The infiltrate is an admixture of lymphocytes and plasma cells.
){kind=link}
Many areas are totally devoid of follicular epithelium.
){kind=link}
Germinal centers are present but sparsely distributed.
){kind=link}
Sclerosis of the thyorid gland can occur in both benign and malignant settings. Examples of benign conditions include the fibrosing variant of Hashimoto thyroiditis and Reidel's disease. Although in the past, they were thought of as possibly related entities, they are now considered distinct clinicopathologic entities. Malignant neoplasms of the thyroid such as papillary thyroid carcinoma and anaplastic carcinoma can elicit extensive sclerosis of the thyroid parenchyma (Baloch).
The gross appearance of fibrosing variant of Hashimoto disease is firm, enlarged and fibrotic gland. Unlike Riedel disease, the fibrosis does not extend to beyond the gland. Histologically, dense keloidal fibrosis replaces much of the gland, and the remaining parenchyma is composed of atrophic follicles with features of Hashimoto thyroiditis (e.g. lymphoplasmatic infiltrate and follicles with oncocytic epithelium).
In Riedel's disease, the fibrosis extends into the surrounding soft tissues and the fibrous bands can be seen intermingling with skeletal muscle, nerve and fat. Reidel's can occur in isolation or as part of a multifocal systemic fibrosis process. It is currently hypothesized that Riedel's may be a manifestation of IgG4-related systemic disease,(Dahlgren) a recently recognized syndrome characterized by mass-forming lesions in exocrine glands and extranodal tissue (most frequently pancreas, biliary duct, and lacrimal gland), elevated serum IgG4 level, and good response to steroids.
In addition, among cases of Hashimotos' thyroiditis, those with IgG4 positive plasma cells showed a higher grade of stromal fibrosis, lymphoplasmacytic infiltration, and follicular cell degeneration than non-IgG4 thyroiditis (Li). These investigators also found that IgG4 thyroiditis is generally associated with males and is often significantly associated with shorter disease duration before surgery.
This variant comprises approximately 10% of all Hashimoto thyroiditis cases and generally affects the elderly (Barnes). This variant may be associated with severe pressure symptoms in the neck and a firm thyroid gland, often with a recent enlargement of a goiter.
→The key difference between the fibrosing variant of Hashimoto thyroiditis and Riedel thyroiditis is that the latter extends past the gland into the surrounding soft tissue.
Baloch ZW, Feldman MD, LiVolsi VA. Combined Riedel's Disease and Fibrosing Hashimoto's Thyroiditis: A Report of Three Cases with Two Showing Coexisting Papillary Carcinoma. Endocr Pathol. 2000 Summer;11(2):157-163.
Barnes L. Surgical Pathology of Head and Neck Third Edition Vol 2. Informa Healthcare; 2008: 1680.
Dahlgren M, Khosroshahi A, Nielsen GP et al. Riedel's thyroiditis and multifocal fibrosclerosis are part of the IgG4-related systemic disease spectrum. Arthritis Care Res (Hoboken). 2010 Sep;62(9):1312-8.
Li Y, Nishihara E, Hirokawa M, Taniguchi E, Miyauchi A, Kakudo K. Distinct clinical, serological, and sonographic characteristics of hashimoto's thyroiditis based with and without IgG4-positive plasma cells.J Clin Endocrinol Metab. 2010 Mar;95(3):1309-17.