
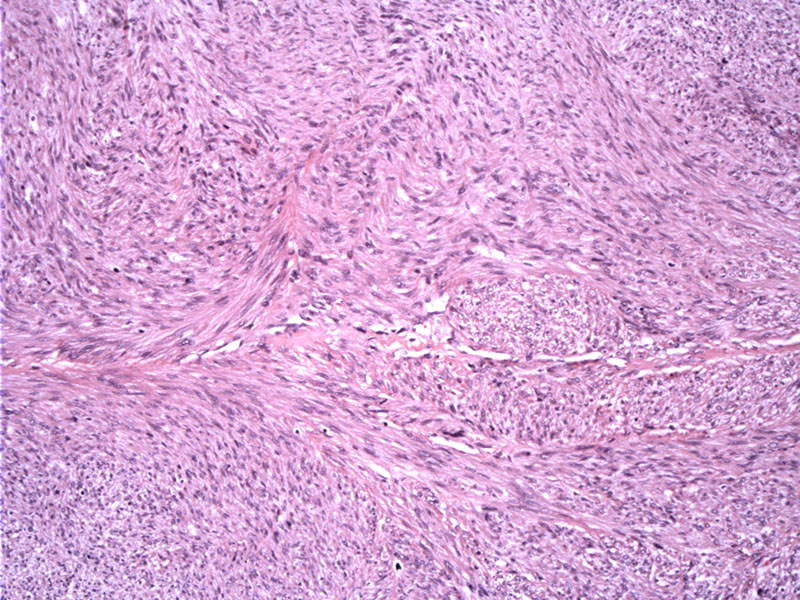
Leiomyosarcomas are characterized by leiomyosarcomas are characterized by fascicles of tumor cells with blunt-ended "cigar-shaped" nuclei.
){kind=link}
Histologically, leiomyosarcomas are characterized by fascicles of tumor cells with blunt-ended "cigar-shaped" nuclei. The nuclei are usually centrally located in better differentiated areas, but in poorly-differentiated frankly sarcomatous regions, the nuclei may be pleomorphic, hyperchromatic and lose their central location. Mitotic figures are common, as well as areas of necrosis, hemorrhage and degeneration.
){kind=link}
Case 2: This different case also contains cigar shaped nuclei of the neoplastic cells as well as scattered enlarged pleomorphic cells.
){kind=link}
Myxoid degeneration (bottom) can be appreciated.
){kind=link}
CT scan imaging demonstrates a large retroperitoneal leiomyosarcoma. The mass is seen as a soft tissue mass in the left retroperitoneum, adjacent to the inferior border of the spleen with a low attenuating center consistent with necrosis.
){kind=link}
Leiomyosarcomas (LMS) are malignant neoplasms that arise from smooth muscle and account for 5-10% of all soft tissue tumors. They are very uncommon in children and tend to affect adults (median age of 60).
Soft tissue leiomyosarcoma is usually subdivided into 3 groups for treatment and prognostic purposes :
(1) LMS of somatic soft tissue
(2) cutaneous LMS
(3) LMS of vascular origin.
Other (very rare) categories may include LMS arising in immunocompromised patients and LMS of bone (Weaver).
LMS arising in viscera such as uterus and GI tract are actually much more common than those arising from somatic soft tissue, and are discussed elsewhere. LMS of somatic soft tissue is thought to arise from smooth muscle lining small veins and unlike LMS arising from large vessels, these lesions do not cause vascular compromise (obstruction, thromboemboli, etc..) (Farshid).
The most common location for LMS arising in somatic soft tissue is the retroperitoneum (50% of cases). Other sites include soft tissues of the extremities, trunk and intra-abdominal locations. Cutaneous LMS is thought to be derived from the pilar arrecti. Vascular LMS usually arises in low pressure systems such as veins (e.g. IVC, pulmonary artery).
LMS in immunocomprised hosts may be related to EBV infection. LMS of bone is extremely rare and LMS from soft tissue directly invading bone must first be ruled out. LMS of bone is thought to arise from the smooth muscle cells lining the intraosseous vessels or possibly from pluripotent mesenchymal cells (Weaver).
Their IHC profile includes positivity for smooth muscle markers (e.g. SMA), and positivity for desmin in 50%-100% of cases.
LMS is a largely resistent to chemotherapy and radiation. Surgery is the mainstay of treatment.
Prognosis is poor and at least in those in the retroperitoneum, varies significantly according to the tumor grade. 1/3 of patients have evidence of metastasis at time of diagnosis, possibly as a result of their close relationship with vessels i.e. the venous system, faciliating dissemination. Unfavorable indications include size of tumor and stage of disease (Mankin).
Farshid G, et al. Leiomyosarcoma of somatic soft tissues: a tumor of vascular origin with multivariate analysis of outcome in 42 cases. Am J Surg Pathol. 2002 Jan;26(1):14-24.
Mankin HJ, et al. Leiomyosarcoma of somatic soft tissues. Clin Orthop Relat Res. 2004 Apr;(421):225-31.
Weaver MJ, Abraham JA (2007). Leiomyosarcoma: ESUN article. Available at: sarcomahelp.org/learning_center/leiomyosarcoma.html