
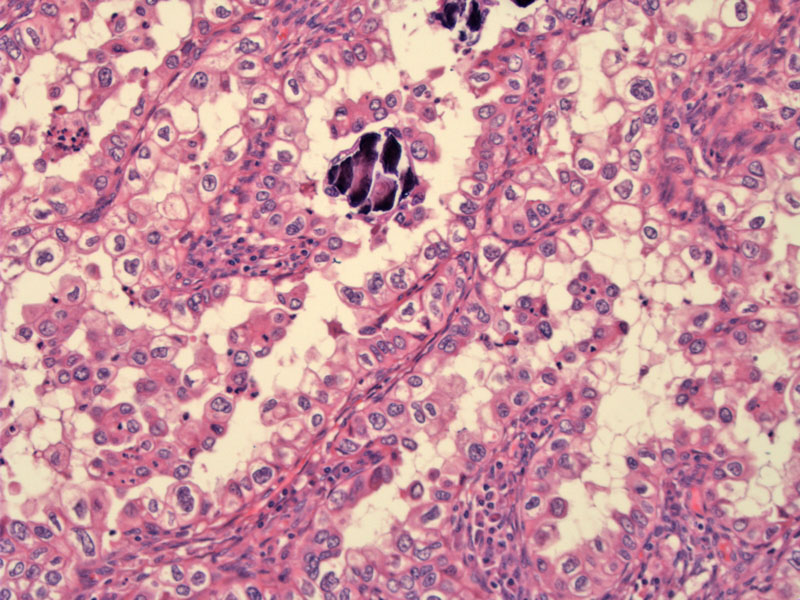
Slender papillae are lined by malignant clear cells with abundant clear cytoplasm. Note the marked nuclear pleomorphism and prominent nuclear membranes. Psammomatous calcification is seen.
){kind=link}
At the carcinoma-myometrial interaface, tubulocystic structures are lined by malignant clear cells. Hobnail cells are frequently seen in clear cell carcinom, and there are some at the lower border of the cystic structure.
){kind=link}
Malignant clear cells are percolating through the myometrium. The nuclei are enlarged and somewhat angulated. A binucleate nucleus is seen.
){kind=link}
Another case demonstrates classic areas of clear cell change growing in a largely solid pattern. Note that the cell membranes are prominent, a characteristic feature of clear cells.
){kind=link}
Bizarre and multinucleated macrosized cells are easily found in this malignancy. Note that clear cells can also exhibit lightly stained acidophilic cytoplasm.
){kind=link}
Other areas of this tumor demonstrate confluent islands of necrosis surrounding malignant cells. Note that these malignant cells are forming a cuff around the blood vessels, which feed the tumor.
){kind=link}
Carcinoma-myometrial interface shows a ragged pushing tumor with a lymphocytic reaction. Note that not all the cells in this particular tumor demonstrate the classic clear cell morphology. These are two main reasons for this: (1) clear cells may stain with acid stains and appear eosinophilic and (2) clear cell carcinoma may coexist with papillary serous adenocarcinoma.
){kind=link}
Clear cell adenocarcinoma of the endometrium falls under the category of type II endometrial adenocarcinomas. Similar to papillary serous endometrial adenocarcinoma (the prototype of type II), these tumors are high-grade with aggressive biologic behavior. In contrast to papillary serous carcinoma, however, they are p53 negative and do not have the propensity to involve peritoneal surfaces. Clear cell carcinoma and papillary serous endometrial carcinoma may occasionally co-exist.1,2
The classic clear cell histology demonstrates glands or papillae lined by a single layer of polygonal cells with clear cytoplasm and enlarged atypical nuclei. The most common architectural pattern is papillary, however, solid and tubulocystic is often seen as well. Frequently, there is a mixture of patterns.
Clinical features are similar to those of papillary serous endometrial adenocarcinoma, as both belong in the type II endometrial carcinoma category. These tumors occur in postmenopausal women (usually older than 60) without a history of hyperestrogenism. Furthermore, unlike clear cell carcinoma of the vagina and cervix, there is no history of DES exposure. They typically present with post-menopausal bleeding.
Surgical staging of uterine cancers consists of total hysterectomy, bilateral salpingo-oophorectomy, pelvic and peri-aortic lymph node dissection, and pelvic washings. As these tumors have a high rate of spread and recurrence, adjuvant pelvic radiation therapy is often employed, and various chemotherapy regimens are undergoing trials.
Survival is much poorer than for stage-matched endometrioid adenocarcinoma due to the high rate of spread as well as high frequency of recurrence. A study reported an overall survival of 42% and 39% at 5 and 10 years, respectively.2
♥ Clear cell carcinoma falls under the category of type II endometrial carcinoma, of which the prototype member is serous carcinoma.
♥ Clear cell carcinoma of the endometrium is not associated with DES exposure in utero, unlike clear cell carcinoma of the cervix and vagina.
1 Nucci MR, Oliva Esther. Gynecologic Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier: 2009: 250.
2 Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 662-3.
3 Sternberg SS, ed. Diagnostic Surgical Pathology.4th Ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2004: 2487.