
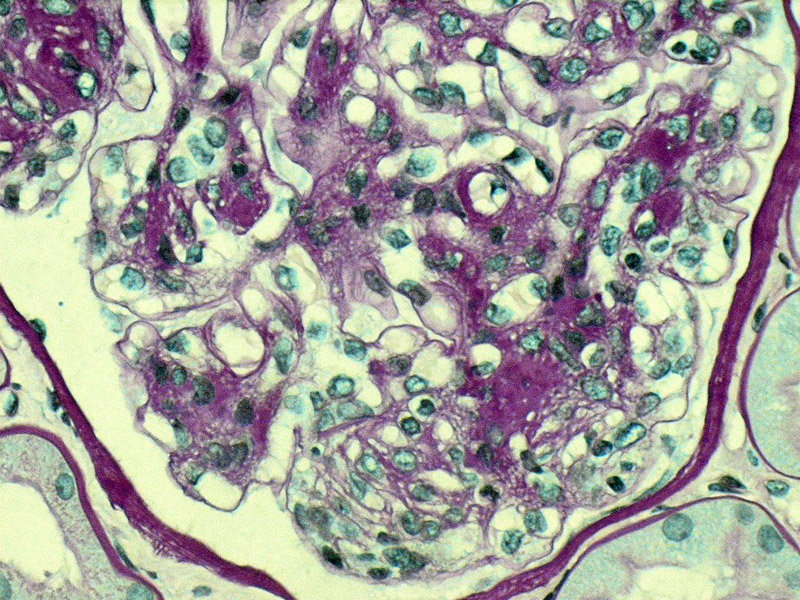
Early mesangial sclerosis is seen in this PAS stained glomerulus. This sclerosis can be diffuse or nodular. The nodular form is also called Kimmelstiel-Wilson nodular sclerosis (see example below). These lesions are initially hypercellular but become hypocellular in time.
){kind=link}
Trichrome shows advanced interstitial fibrosis and atrophy, with concordant sclerosis of the glomerulus. An insudative lesion is seen as a red crescent, compatible with a fibrin cap. Fibrin caps result from accumulation of hyaline material.
){kind=link}
Hyalinization of tubules is characteristic, as well as hyalinization of both the efferent and afferent arterioles. Furthermore, the tubular basement membrane are thickened with a laminated appearance.
){kind=link}
The nodular accumulation of mesangial matrix is rather profound here, resulting in a large round eosinophilic Kimmelstiel-Wilson nodule (6:00).
){kind=link}
Linear IgG on immunofluorescence can often be seen in diabetic nephropathy. The IgG deposits are not only along the glomerular basement membrane but may also be detected along tubular basement membranes and the glomerular mesangium.
){kind=link}
Again, linear staining for IgG and albumin is seen in both the GBM and TBM in this renal core biopsy.
){kind=link}
Diffusely thickened glomerular basement membranes is another characteristic feature which is appreciated on electron microscopy.
){kind=link}
Mesangial sclerosis encroaches on the capillary lumens located in the upper left corner
){kind=link}
Obvious Kimmelstiel-Wilson nodules can be appreciated on this PAS stain. These nodular acellular lesions lie within the mesangial core -- still patent capillary loops can be seen overlying the nodules.
){kind=link}
Heavy and diffuse deposition of hyaline material is seen in this glomerular tuft.
){kind=link}
Yet another case demonstrating nodule increase in mesangium (mesangial expansion) with formation of nodules. The interstitium shows some fibrosis, with tubular atrophy and nonspecific small collections of lymphocytes.
){kind=link}
Renal failure due to diabetic nephropathy is the most common cause of end stage renal disease in this country. Advanced renal damage or renal failure is seen in up to 40% of both Type I and Type II diabetics (Kumar).
Diabetes damages the microvasculature. It is a disease which affects both glomeruli and vessels. Glomeruli acquire an increase in mesangial matrix which can be either diffuse, nodular, or both. When there is nodular accumulation, these areas are referred to as "Kimmelstiel-Wilson" lesions. The glomerular basement membrane can be uniformly and markedly thickened.
Insudative lesions (i.e. hyaline deposits) are a feature of this disease. When these hyaline deposits are located beneath the parietal epithelium of Bowman's capsule, it is referred to as "capsular drops", and when located within glomerular tuft, it is known as "fibrin caps".
The hallmark of diabetic nephropathy is proteinuria. Initially, patients develop microalbuminuria, and as the disease advances, proteinuria in the nephrotic range is seen. Retinal exams are helpful in evaluating microvasculature (Zhou).
Strict control of blood glucose can delay progression of renal disease. ACE inhibitors, and anti-hypertensive medications can also be beneficial. In advanced renal disease, dialysis and renal transplantation may be required.
Proteinuria is an ominous sign and usually appears 12-22 years after the clinical onset of diabetes -- chronic renal failure leading to end stage renal disease or death occurs within 4-5 years.
Kumar V, Abbas AK, Fausto N. Robbins and Cotran Pathologic Basis of Disease. 7th Ed. Philadelphia, PA: Elsevier; 2005: 990-2.
Zhou M, Magi-Galluzzi, C. Genitourinary Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elvesier; 2006: 359-362.