
CT scan shows a large cavitary lung mass in the left lower lobe.
){kind=link}
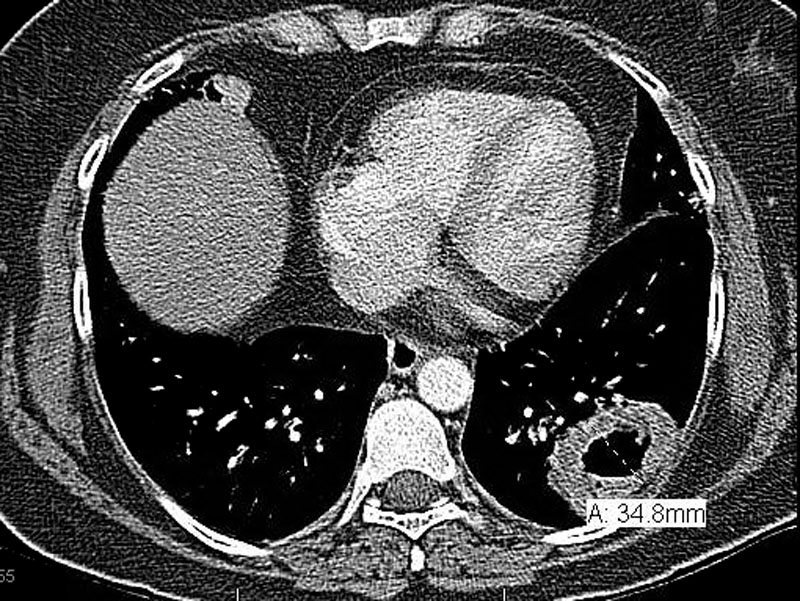
CT scan on the same patient shows hilar, subcarinal, and mediastimal adenopathy.
){kind=link}
Neoplastic cells with abundant cytoplasm grow in sheets.
){kind=link}
There is a robust inflammatory infiltrate interspersed with the malignant growth.
){kind=link}
This moderately differentiated area shows tumor cells with clearly pleomorphic nuclei, but abundant cytoplasm and hints of intercellular bridges.
){kind=link}
Pallisading around vessels can be appreciated here.
){kind=link}
There is marked desmoplasia and focal keratin pearls (right lower image).
){kind=link}
Again, note the extensive desmoplasia. The neoplastic cells are staining quite darkly here.
){kind=link}
The tumor arises centrally and involves both sides of the bronchial cartilage wall.
){kind=link}
This example demonstrates an odd growth pattern for a SCC, where tumor cells undermine alveolar epithelial cells.
){kind=link}
Squamous cell carcinoma (SCC) accounts for approximately 1/3 of all non-small cell lung carcinomas (NSCLCs). Defined as a malignant epithelial tumor with squamous differentiation, SCC can be well, moderately or poorly differentiated. Well-differentiated SCC contains sheets of neoplastic cells with the following features: (1) abundant pink cytoplasm (2) distinct cell borders with intercellular bridges and (3) areas of keratinization. As the tumor increases in grade, these aforementioned features are less obvious and there is an increase in mitotic activity, cytologic atypia, necrosis and hemorrhage. Central comedo necrosis may be present as well. Variants include: papillary, SCC, spindle cell SCC, clear cell changes and basaloid SCC.
SCC most often arises centrally from first to third order bronchi, although as many as 1/3 may arise peripherally (Zander, Fletcher). Approximately 10% of SCC undergo central cavitation and thus, may mimic certain fungal and bacterial infections radiologically.
SCC is strongly associated with smoking, and due to its preferred central location, patients present with cough, shortness of breath and hemoptysis. Hypercalcemia can occur as the tumor elaborates PRP (parathyroid-hormone related protein).
Post-obstructive pneunomia can is quite common (Zander). Because of their central location, SCC can sometimes be diagnosed with non-invasive methods such as cytologic examination of sputum, BAL (bronchoalveolar lavage) fluid, bronchiole brushings and washings.
In the past decades, SCC was the most common NSCLC due to smoking habits. As smoking has decreased among the population, adenocarcinoma is now the most common NSCLC.
Surgical resection remains the single most successful option. Up to 70% present with locally advanced or metastatic disease at diagnosis and in such cases, chemotherapy and/or radiation may be beneficial. Adjuvant chemotherapy may be indicated for those with resected stages IIA through IIIA NSCLC.
Although SCC grows more rapidly compared to other types of NSCLC, they tend to metastasize later.
2/3 of SCC is located central and 1/3 located peripherally.
Presents with cough, hemoptysis and possibly hypercalcemia (due to PRP elaboration by SCC).
Graded into well, moderately or poorly differentiated depending on degree of squamous differentiation.
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 185.
Zander DS, Farver CF. Pulmonary Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elvesier; 2008: 553.