
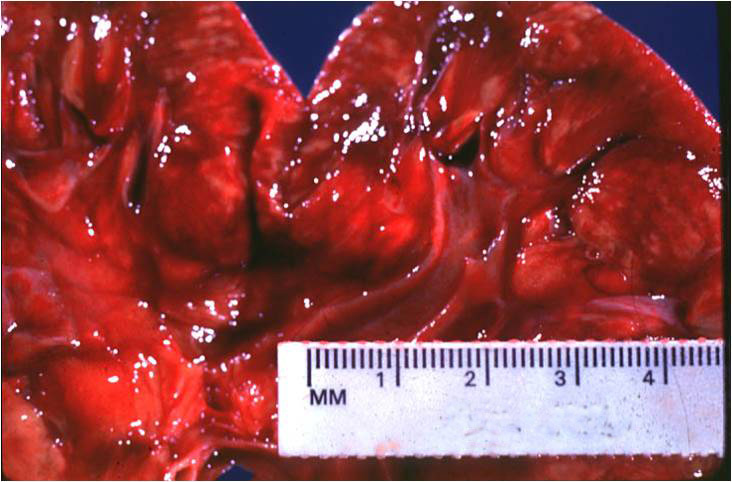
The renal cortex shows erythema but also variegated areas of pallor, which represent foci of acute inflammation.
){kind=link}
This glomerulus is surrounded by a dense neutrophilic infiltrate.
){kind=link}
Collections of neutrophils fill the tubular lumen, which appears injured. The suppurative inflammation is also within the adjacent interstitium.
){kind=link}
Acute pyelonephritis results from a bacterial infection of the kidney. Most pediatric cases are males, while most adult cases are females. Infection can occur either by the ascending route, or via the bloodstream. The former is most often due to E. Coli, although other bacteria such as Proteus, Klebsiella, and Enterbacter may be the causative agent. Hematogenous pyelonephritis most often affect debilitated patients and the immunosuppressed. Staphylococcal or fungal infections may spread to the kidney from distant foci in the bone or skin.
There is a wide spectrum, from a mild illness to sepsis. Typical presenting signs include fever, elevated WBC count and flank pain. WBCs in the urine is also typical.
Patients can be divided into complicated and uncomplicated types. Those with complicated pyelonephritis require blood cultures and urinary tract imaging, preferably a CT scan. Patients with moderate, uncomplicated pyelonephritis can be managed as outpatients with either a fluoroquinolone or trimethoprim/sulfamethoxazole. Patients with severe, but uncomplicated pyelonephritis may require short-term hospitalization and intravenous antibiotics.
Complications that may result include a perinephric abscess and urosepsis. Particularly in the presence of obstruction (stone, tumor, bladder neck obstruction, enlarged prostate), acute pyelonephritis can be recalcitrant to treatment, and may progress to renal abscess.