
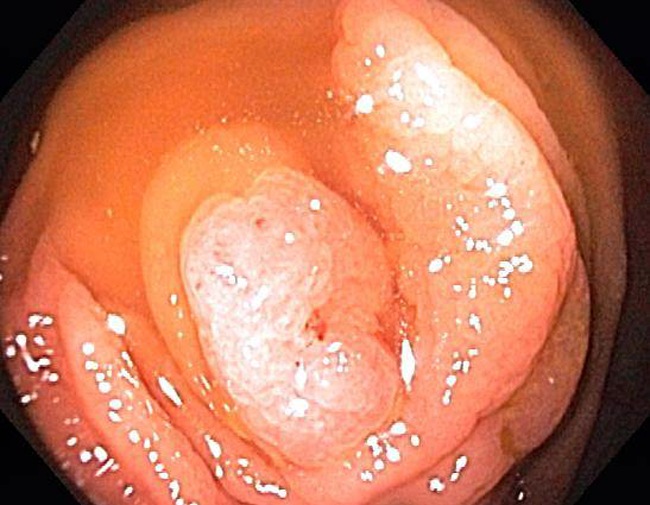
Endoscopic image of a hyperplastic appendiceal polyp demonstrates a sessile lesion.
){kind=link}
A microscopic image of the biopsy demonstrates hyperplastic glands. The glands are elongated with a serrated profile. Note that adenomatous change was lacking, thus, distinguishing this lesion from an adenoma. Unfortunately, there is knife chatter artifact distorting this image, however, due to the rarity of this lesion, another image is not available at this time.
){kind=link}
Hyperplastic lesions of the appendix come in two forms: diffuse hyperplasia and hyperplastic polyps. Hyperplastic polyps are localized sessile masses that are morphologically similar to those found in the colon; they are quite rare. In contrast, diffuse hyperplasia is more common and consists of nonpolypoid hyperplasia affecting the mucosa. Both lesions demonstrated elongated tubules with serrations.1
It is fascinating to note that the presence of hyperplastic lesions in the appendix is significantly associated with the co-existence of adenocarcinoma exists elsewhere in the GI tract. In a study conducted by Younes, 17 out of 23 appendices with mucosal hyperplasia were associated with colonic adenocarcinoma (located predominantly in the right colon).2
It is important to differentiate hyperplastic lesions from villous or serrated adenomas in the appendix, as appendiceal adenomas appear to be much more aggressive lesions in the appendix when compared to their counterparts in the colon. Rubio (2004) conducted a study of villous and serrated adenomas and found that 11 of 16 villous adenomas and 4 of 10 serrated adenomas had demonstrated invasive carcinomas of the appendix when the organ was thoroughly sampled.3 The key difference between the two is the dysplastic/adenomatous change is seen in adenomas and absent in hyperplastic lesions. Note that if both hyperplastic and dyplastic epithelium is identified, the term "mixed hyperplastic polyp/serrated adenoma" is sometimes used.
True incidence may be underestimated as they are usually not seen endoscopically and are thus discovered on appendectomy done for other reasons. Furthermore, it is common practice in pathology to submit several representative sections of an appendix and thus, the entire mucosa is not usually examined.
Although further research needs to be conducted in this area, it appears that epithelial neoplasms of the appendix exhibit a similar dysplastic-neoplastic sequence found in the colon. Hyperplastic polyps may evolve into serrated adenomas, which then may progress into invasive adenocarcinomas (most often, the mucinous type). Hyperplastic and adenomatous lesions in the appendix is much more aggressive than those found in the colon, and as mentioned above, hyperplastic lesions in the appendix is curiously associated with colonic adenocarcinomas.
1 Odze RD, Goldblum JR, Crawford, JM. Surgical Pathology of the GI Tract, Liver, Biliary Tract, and Pancreas. Philadelphia, PA: Elsevier; 2004: 473-4.
2 Younes M, Katikaneni PR, Lechago J. Association between mucosal hyperplasia of the appendix and adenocarcinoma of the colon. Histopathology. (1995)Jan;26(1);33-7.
3 Rubio CA. Serrated adenomas of the appendix. J Clin Pathol 2004;57:946-949.
Please visit our other cases for epithelial neoplasms for the appendix:
- Serrated adenoma
- Low grade mucinous neoplasm