
A proliferation of bland ovoid cells in a fibromyxoid and focally hyalinized stroma can be appreciated. These cells are S100 positive.
){kind=link}
A hallmark feature is the peripheral shell of lamellar bone.
){kind=link}
The cells have vesicular round-to-oval nuclei, are evenly spaced with low mitotic activity. Nuclei are relatively uniform and nucleoli are not prominent. The stroma transitions to fibromyxoid to collagenous and hyalinized.
){kind=link}
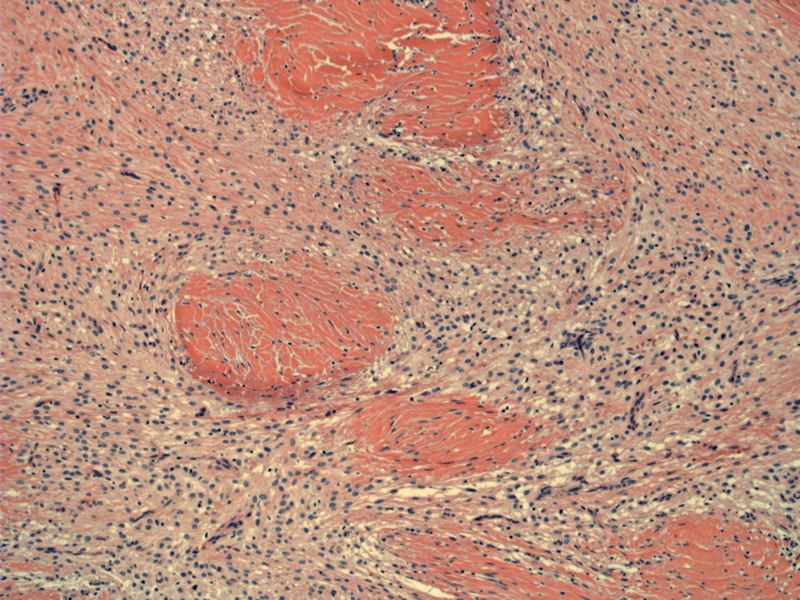
This is another area of metaplastic bone, which forms an incomplete shell here.
){kind=link}
Ossifying fibromyxoid tumor of soft parts (OFMT) is a recently characterized mesenchymal neoplasm that usually presents as a subcutaneous nodule in adults (Fletcher).
Histologically, there is a peripheral shell of bone (seen in 70% of cases) with a lobular growth of small round cells separated by fibrous septae. The cells are regularly spaced with no overlap. The stroma is fibromyxoid and can be focally hyalinized. Malignant features include increased cellularity with nuclear crowding/overlap, necrosis, vascular invasion and mitotic activity greater than 2 MF per 50 HPF (Folpe).
The majority of the tumors (60% to 94%) stain with S-100 and a smaller subset stain focally for cytokeratins, SMA, desmin. A few tumors may even express nerve sheath markers such as CD57 and GFAP (Folpe, Miettinen).
These arise in a wide variety of locations, with a slight preference for the lower extremity. A long history of a slow growing painless mass may be elicited.
Resection with negative margins.
When strictly defined by Miettinen et al. as a tumor with the following features: (1)lobular architecture (2) predominantly epithelioid cell morphology (3) low level of atypia (4) corded and trabecular growth patterns (5) moderate amounts of myxocollagenous matrix and (6) focal peripheral metaplastic bone formation, their retrospective review of 104 cases found that the great majority of OFMT behaved in a benign fashion. Only 9 of 41 cases available for follow-up had local recurrences and there were no metastases.
Other studies, however, found higher instances of metastases, possibly due to differences in diagnostic criteria. For example, in study of 59 cases with 41 available for followup, 11 patients (27%) experienced one or more recurrences and one patient had probable metastases (Enzinger 1989). Likewise, followup in 51 cases showed local local recurrences in 9 patients and metastases in 8 patients (Folpe 2004). Folpe in his textbook goes as far as stating that in histologically benign OFMTs, distant metastasis may be seen in 6% of cases whereas histologically malignant OFMTs lead to distant metastasis in 60% (Folpe 2010).
Furthermore, there have been convincing cases of pulmonary metastases of the so-called malignant OFMTs documented in the literature (Sarraj, Suehiro).
Clearly, there is some debate and varying among experts regarding the benign versus malignant nature of this rare tumor and the exact criteria to separate the two. Currently, this tumor may currently be best classified as of uncertain or intermediate malignant potential.
• Fibrous : Myositis Ossificans
Enzinger FM, Weiss SW, Liang CY. Ossifying fibromyxoid tumor of soft parts. A clinicopathological analysis of 59 cases.Am J Surg Pathol. 1989 Oct;13(10):817-27.
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 1573.
Folpe AL, Inwards CY. Bone and Soft Tissue Pathology: Foundations in Diagnostic Pathology Philadelphia, PA: Elsevier; 2010: 285-6.
Folpe AL, Weiss SW.Ossifying fibromyxoid tumor of soft parts: a clinicopathologic study of 70 cases with emphasis on atypical and malignant variants. Am J Surg Pathol. 2003 Apr;27(4):421-31.
Miettinen M, Finnell V, Fetsch JF. Ossifying fibromyxoid tumor of soft parts--a clinicopathologic and immunohistochemical study of 104 cases with long-term follow-up and a critical review of the literature.Am J Surg Pathol. 2008 Jul;32(7):996-1005.
Sarraj A, Duarte J, Dominguez L, Pun YW. Resection of metastatic pulmonary lesion of ossifying fibromyxoid tumor extending into the left atrium and ventricle via pulmonary vein. Eur J Echocardiogr. 2007 Oct;8(5):384-6. Epub 2006 Jun 8.
Suehiro K, Pritzwald-Stegmann P, Lee KM, Teoh HH, Alison PM. Mediastinal and pulmonary metastases of malignant ossifying fibromyxoid tumor. Ann Thorac Surg. 2006 Jun;81(6):2289-91.