
Proliferative endometrium with glandular and stromal breakdown is the most common pattern in anovulatory cycles. In chronic anovulation cycle, proliferative glands become distorted and irregularly dilated.
){kind=link}
Venules are dilated and often thrombosed. Due to the chronic estrogenic stimulation, estrogen-induced epithelial changes such as ciliated cells may be seen. The two glands in this image are lined by ciliated cells.
){kind=link}
Glands are variably sized and haphazardly arranged.
){kind=link}
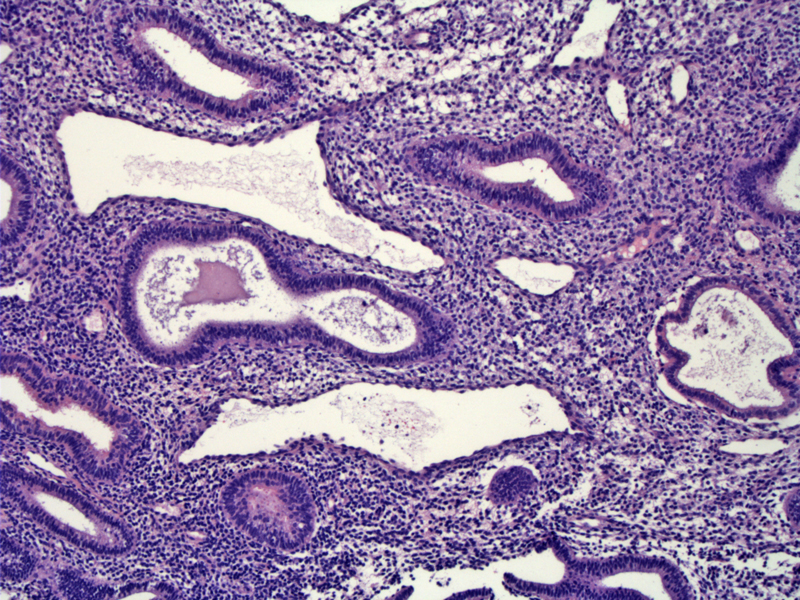
Large cystically dilated proliferative glands are seen in this is a patient with polycystic ovary disease.
){kind=link}
This different example shows variably cystic glands, with a surface showing incipient breakdown. There is eosinophilic change to the surface epithelium as well as lifting of the epithelium.
){kind=link}
Adjacent to the prior area is evidence of breakdown consisting of some free floating aggregates of stromal condensation and sloughed eosinophilic surface epithelium.
){kind=link}
An organizing thrombus is seen in another fragment, along with neutrophils admixed within the denuding surface epithelium.
){kind=link}
The main effect of estrogen on endometrium is to stimulate proliferation of glands, stroma and endothelium. The degree of mitotic activity is a good measure of proliferative activity. In anovulation, the endometrium is continuously exposed to estrogen because ovulation does not occur, thus the corpus luteum does not form and progesterone is not produced. This leads to a pattern of continuous unrelieved proliferation. Eventually, the endometrium can no longer support the proliferative glands and breaks down. The amount glandular and stromal breakdown will vary from extensive to focal.
Histologically, one sees stromal and glandular breakdown superimposed on a proliferative pattern, so-called "anovulatory bleeding". It is important not to label this as menstrual bleeding. Menstrual bleeding occurs at the end of a normal menstrual cycle and one sees secretory glands (demonstrating secretory exhaustion) with glandular and stromal breakdown.
With prolonged chronic estrogen exposure, the proliferating glands will become haphazardly oriented and vary in shape and size, thus leading to the descriptive term disordered proliferative endometrium.
Anovulatory cycles commonly occur in perimenopausal and perimenarchal women. Anovulatory cycles are a cardinal feature of polycystic ovarian syndrome. Obesity is also associated with anovulatory cycles as high circulating estrone produced by adipose tissue suppresses pituitary gonadotropin secretion.
Treatment of anovulation is tailored to the patient's goals. If the patient's goal is to reduce the risk of future endometrial hyperplasia, exposure to progesterone whether in medications or implants is recommended. If the patient's goal is ovulation and pregnancy, treatment with ovulation induction agents such as clomiphene citrate is recommended.
Chronic anovulation is associated with unpredictable menstrual patterns as well as menstrual patterns that can result in significant anemia. In the long term, chronic anovulation can result in endometrial hyperplasia and ultimately endometrial adenocarcinoma.
Mazur MT, Kurman RJ. Diagnosis of Endometrial Biopsies and Curettings. New York, NY: Springer; 2005: 109-113.
Robboy SJ, Anderson MC, Russell P. Pathology of the Female Reproductive Tract. London, UK: Churchill Livingstone; 2002: 267-8.