
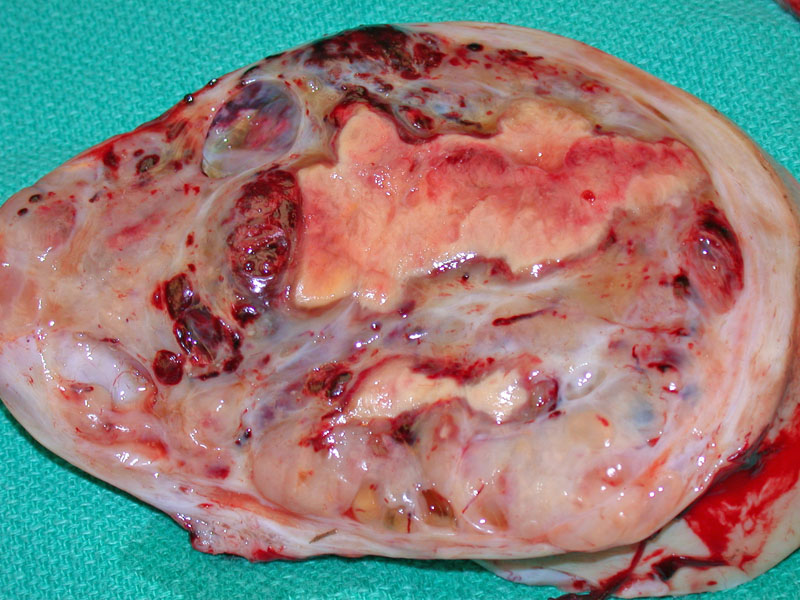
Grossly, the tumor is similar to the adult type, consisting of solid and cystic areas. The tumors can range from 2.5 to 32 cm. The solid areas are frequently tan-yellow with a nodular rubbery cut surface, and the cysts often contain serous or serosanguineous fluid. This juvenile granulosa cell tumor is bulky and contains both cystic and solid components admixed with hemorrhagic areas and zones of yellow necrosis.
){kind=link}
A closer look reveals the fleshy rubbery nature of the solid component with superimposed necrosis (yellow zone).
){kind=link}
A tan nodule (solid component) was located on the inside surface of a cystic area within the tumor.
){kind=link}
Microscopically, the tumor cells are arranged in a nodular, solid or cystic growth pattern. In this image, a solid diffuse sheet of tumor cells is seen.
){kind=link}
The most characteristic feature of juvenile GCT is the formation of macrofollicles, which contain mucinous material, vary widely in size and shape. Some are rounded and small, while others are large and irregularly shaped. In contrast to adult GCT, Call-Exner bodies are rare.
){kind=link}
The tumors cells in juvenile GCT differ from those of the adult type. The cells are larger, polygonal with moderate to abundant cytoplasm, which can be vacuolated, as seen here. The nuclei round or ovoid, hyperchromatic and do not contain grooves (whereas this is characteristic in adult GCT). The background may be edematous or myxoid.
){kind=link}
The tumor cells here are arranged in a ribboning or trabecular pattern. Note the small follicles lined by granulosa cells, some of which even look hobnailed. The tumor cells are polygonal, with hyperchromatic nuclei. There is mild cytologic atypia, which is not uncommon. Not though found here, bizarre nuclei and severe atypia may be seen, which does not correlate with prognosis.
){kind=link}
Focal or extensive lutenization is commonly found in juvenile GCT (but rare in adult GCT). This image demonstrates a luteinized juvenile granulosa cell tumor, consisting of enlarged cells with abundant vacuolated cytoplasm. In other luteinized cells (not shown here), the cytoplasm is more eosinophilic.
){kind=link}
Juvenile granulosa cell tumor (GCT) is a variant of granulosa cell tumor with distinct clinicopathologic features. They can occur in a wide age range (from infancy to adulthood), but the majority occur in infants, children and adolescents.
For example, juvenile granulosa cell tumors exhibit a macrofollicular, solid or cystic growth pattern, whereas the microfollicular and insular pattern common in the adult type is not usually seen or just focally present. Furthermore, the composite tumor cells are polygonal or spindled in shape with abundant eosinophilic cytoplasm, whereas adult granulosa tumor cells are usually round with pale cytoplasm. Luteinization is a common finding, which luteinized cells are found in only 1% of adult granulosa cell tumors.1
Overall, both the adult and juvenile granulosa cell tumors have a good prognosis, but juvenile types fare even better. Very late recurrences, common to the adult type, are rare in the juvenile type. In juvenile GCT, most recurrences happen within 3 years from initial diagnosis.
For those who yearn to know more about obscure syndromes, juvenile granulosa cell tumors are found as part of Ollier disease (enchondromatosis) and Maffucci syndrome (multiple enchondromas and hemangiomas).
97% of juvenile GCTs occur before age 30, and 40% occur before age 10. The average age at presentation is 13.2
50-75% of prepubertal girls exhibit precocious puberty as a result of estrogen production by the tumor. The isosexual precocity manifests as breast development, pubic and axillary hair growth and increased bone age. In adolescents or premenopausal women, the estrogen excess causes abnormal vaginal bleeding.
Some patients do not exhibit estrogenic effects and present with a palpable abdominal mass or abdominal pain. Note that an adnexal mass is palpable in over 70% of patients.1 The vast majority of these tumors are unilateral.
Unilateral salpino-oopherectomy, which preserves fertility in this young population, is sufficient in most cases (which are confined to the ovary). Bilateral salpino-oopherectomy and hysterectomy is reserved for stage II disease and beyond. In advanced disease, adjuvant chemotherapy is employed.
Generally excellent as over 95% of cases are confined to the ovary (stage I). Note, however, that prognosis is less favorable starting at stage IC, therefore, one must obtain peritoneal washings to look for malignant cells in the fluid.
• Ovary : Granulosa Cell Tumor
1 Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 591-2.
2 Nucci MR, Oliva Esther. Gynecologic Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier: 2009: 468-472.