
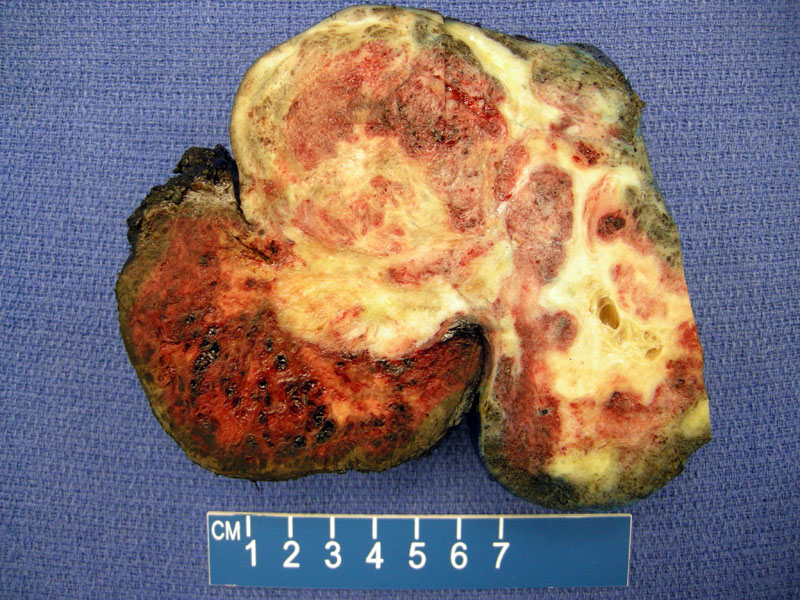
Grossly, this tumor is a bulky mass with solid and cystic tan areas and extensive hemorrhagic. Pure choriocarcinomas are soft, hemorrhagic and necrotic. This tumor showed approximately 20% mature teratoma and 80% choriocarcinoma.
Large zones of hemorrhage are present; cystic areas are also clearly evident.
Microscopically, the tumor is composed of an admixture of syncytiotrophoblasts and cytotrophoblasts. Syncytiotrophoblasts have abundant dense eosinophilic and occasionally vacuolated cytoplasm with clusters of hyperchromatic nuclei. Syncytiotrophoblasts are terminally differentiated and thus, are incapable of cell division (no mitotic figures). Cytotrophoblasts are round to polygonal cells with a single centrally placed vesicular nucleus and distinct cell membranes. Mitotic figures are common and often atypical. Intermediate trophoblasts are rarely found and they are large round or polygonal cells with one or two nuclei (binucleate).
Large zones of fresh hemorrhage dissect through discohesive synctiotrophoblasts and cytotrophoblasts. .
HCG will strongly stain the cytoplasm of syncytiotrophoblastic cells. After definitive therapy, monitoring serum HCG levels is a good way to monitor for recurrence.
A mature teratoma component (squamous epithelium) is admixed with the choriocarcinoma. Pure ovarian choriocarcinomas are extremely rare, but represents a component encountered in up to 20% of mixed germ cell tumors of ovary.
Pure choriocarcinoma is rare and usually seen as a component of a mixed germ cell tumor. In this particular case, the tumor was approximately 20% mature teratoma and 80% choriocarcinoma.
Gestational choriocarcinoma (placental origin) may involve the ovary in advanced stages. Since nongestational (germ cell origin) and gestational (placental origin) choriocarcinomas have different chemotherapy regimens and prognosis, it is important to distinguish between the two entities. If the patient is prepubertal, the diagnosis is easy (nongestational), however, in a woman of childbearing age, either gestational or nongestational choriocarcinoma may occur. The two neoplasms are histologically identical, thus, one must review the clinical history. The presence of a corpus lutem of pregnancy may be helpful. Paternal DNA detected by cytogenetic analysis or flow cytometry would indicate a gestational choriocarcinoma.2 Additionally, in most cases of nongestational choriocarcinoma the tumor is admixed with other neoplastic germ cell elements.
Nongestationmal choriocarcinoma usually affect children and young adults (usually under 20 years of age). The clinical presentation includes abdominal pain, abnormal vaginal bleeding, an adnexal mass and elevated beta-HCG. Pre-pubertal patients may exhibit isosexual precocity. As the tumor is usually hemorrhagic and necrotic, hemoperitoneum is often found during surgery.1,2
The vast majority of the tumors are uilateral, therefore, unilateral salpingo-oopherectomy is usually sufficient if the contralateral ovary and uterus is not involved. Surgery is followed by a chemotherapy regimen. There are only a limited number of reports examining chemotherapy for nongestational choriocarcinoma but complete responses have been reported with the MAC regimen (methotrexate, actinomycin D, cyclophosphamide) used in a manner described for gestational trophoblastic disease (Corakç). BEP regimen (bleomycin, etoposide, cisplatin) used in the manner described for germ cell tumors is preferred by some as an alternative chemotherapy protocol(Corakç). HCG levels can be used to monitor recurrence.
The tumors are rapidly fatal if not treated, with extension into peritoneal cavity and hematogenous spread to lungs and brain. Gestational choriocarcinoma is more responsive to chemotherapy compared to nongestational choriocarcinoma. Survival depends on stage at presentation.
In a review of 31 cases treated with chemotherapy, at the 6-month follow up, survival was 86.1% for those who received adjuvant chemotherapy versus 33.3% for those who received only surgical treatment (Kong).
• Placenta : Gestational Choriocarcinoma
1 Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 608.
2 Nucci MR, Oliva Esther. Gynecologic Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier: 2009: 511-3.
Corakçi A, Ozeren S, Ozkan S, Gürbüz Y, Ustün H, Yücesoy I. Pure nongestational choriocarcinoma of ovary. Arch Gynecol Obstet . 2005 Feb;271(2):176-7.28.
Kong B, Tian YJ, Zhu WW, Qin YJ. A pure nongestational ovarian choriocarcinoma in a 10-year-old girl: case report and literature review. J Obstet Gynaecol Res . 2009 Jun;35(3):574-8.

){kind=link}
){kind=link}
 and syncytiotrophoblasts (multinucleated giant cells) can be seen.', 'micro', '')){kind=link}
){kind=link}
){kind=link}
 was seen in this tumor.', 'micro', '')){kind=link}