
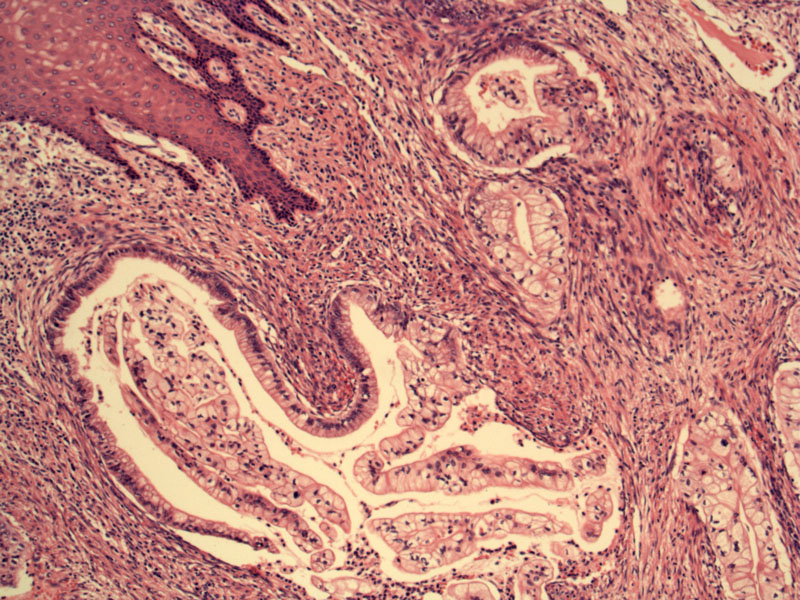
The malignant glands extend deeply into the cervical wall, usually reaching the outer third of the cervical wall. The glands are haphazardly placed and irregularly shaped. The squamous surface epithelium is seen on the upper left.
The cells lining the glands resemble those of benign endocervical glands, with tall columnar cells with plentiful mucin and basally oriented nuclei without. Cytologic atypia is not prominent. Note, however, in contrast to benign endocervical glandular epithelium, the nucleoli are often enlarged.
Although most of the malignant glands in MDA will be bland, there will be focal atypia and focal stromal desmoplasia. Note the contorted shape of these crowded glands, lined by relatively benign appearing mucinous epithelium. The glands appear to elicit a subtle desmoplastic response.
Adenoma malignum, also known as minimal deviation adenocarcinoma (MDA), is so named because of the contrast between its bland highly-differentiated histology and its aggressive biological behavior. MDA is rare, comprising only 1-3% of all cervical adenocarcinomas and is considered a variant of mucinous adenocarcinoma (Nucci).
10-15% of patients with MDA have Peutz-Jeghers syndrome (PJS). PJS is an autosomally dominant inherited condition characterized by hamartomatous polyps in the GI tract and mucocutaneous pigmentation. Persons with PJS also have a higher risk of developing cancers in various anatomic sites. For PJS females, cancers in the reproductive tracts include sex-cord tumor with annular tubules and adenoma malignum. Note that mutations of the tumor suppressor gene STK11 responsible for JPS has been found in sporadic cases of MDA (Fletcher).
MDA may appear histologically similar to a variety of non-neoplastic conditions such as benign endocervical glands, tunnel clusters, adenomymoma (endocervical type), endocervicosis and lobular endocervical glandular hyperplasia. These conditions on the differential diagnosis are much more common, and therefore, must be ruled out before MDA can be diagnosed. Several key features will be helpful in distinguishing MDA from its mimickers. MDA tends to involve the outer third or half of the cervical wall with an abnormal clinical appearance of the cervix; the glands are irregularly shaped, almost leaf-like with focal cytologic atypia, desmoplasia and mitotic activity. The other entities will exhibit some, but not all of these features (Fletcher).
Typically presents with vaginal bleeding or mucoid discharge (Nucci). The peak age at diagnosis is 42, in contrast with conventional endocervical adenocarcinoma which presents at a later age (between 45-54).
Treatment is according to stage and follows the same guidelines as for cervical adenocarcinoma.
Patients tend to present at a higher stage, as the tumor tends to invade deeply into the stroma and metastasize early. Prognosis is significantly worse than conventional endocervical adenocarcinoma. Overall survival rate for stage I tumors is 50% and overall survival rate for all stages is 28% (Nucci, Fletcher).
Nucci MR, Oliva Esther. Gynecologic Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier: 2009: 178-180.
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 705-6.
**Images courtesy of Dr. Lida Crooks, VAMC Albuquerque NM.

){kind=link}
){kind=link}
){kind=link}