
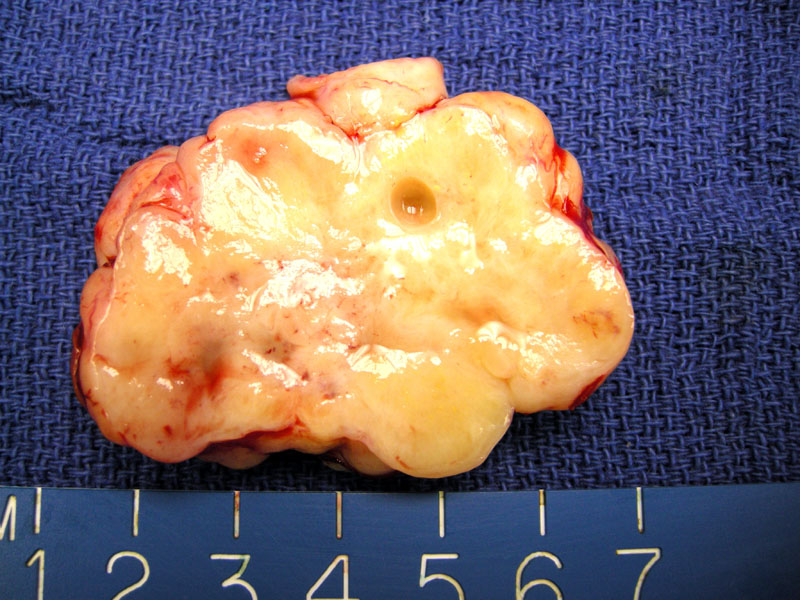
The cut surface of the ovary reveals a solid yellow-tan mass replacing and expanding the ovarian parenchyma.
){kind=link}
Similar to lobular carcinoma of the breast, densely packed cords of relatively uniform cells infiltrate a sclerotic background.
){kind=link}
The lesional cells undermine the surface of ovary and elicit a dense stromal response.
){kind=link}
In this case of metastatic ductal carcinoma, some intervening eosinophilic ovarian stroma (right image) is seen. The lesional cells are not particularly enlarged and are arranged in a vaguely nested pattern.
){kind=link}
Desmoplasia is seen immediately around the malignant cells as a paler background relative to spindled ovarian stroma.
){kind=link}
Breast cancer is the most common tumor to metastasize to the ovary, however, it is usually not clinically evident or clinically significant. In most instances, small or microscopic foci of tumor cells have been found in ovaries removed for therapy (to decrease hormonal stimulation of breast cancer). Thus, adnexal masses in women with breast cancer are more likely to be primary ovarian tumors rather than metastatic cancer from the breast. Exceptionally, ovarian metastases are the initial presenting symptom of a breast carcinoma1
Microscopically, the metastatic tumor resembles either ductal or lobular carcinoma of the breast. Lobular carcinoma, especially those containing signet rings, spread to the ovary much more frequently than ductal carcinomas. However, ductal carcinomas are more common in ovaries because of their the greater overall frequency. Metastatic deposits from ductal and lobular carcinoma are 75% and 25%, respectively.2 In lobular carcinoma, the lesional cells are characteristically arranged in a single-file, short cords, trabeculae or insular pattern; prominent signet ring cells can be termed a Krukenberg tumor. At low power, the single cell infiltration of lobular carcinoma may be extremely difficult to detect. In ductal carcinoma, the lesion forms glandular, papillary or cribriform patterns similar to those seen in the breast.2,3
IHC may reveal a profile similar to that of primary ovarian cancer (CK7+, CD20-, ER and PR positive). GCDFP (gross cystic disease fluid protein, aka BRST-2) may be helpful as it will be immunoreactive in well-differentiated ductal carcinomas and a significant portion of lobular carcinomas. GCDFP is negative in primary ovarian carcinoma.1,3
Most often an incidental finding, however, up to 1/3 of ovaries may be diffusely enlarged or contain nodular foci of metastases. Involvement is bilateral in 60-80% of cases.
1 Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 618-620.
2 Mills SE, ed. Sternberg's Diagnostic Surgical Pathology.4th Ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2004: 2627.
3 Nucci MR, Oliva Esther. Gynecologic Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier: 2009: 545-6.