
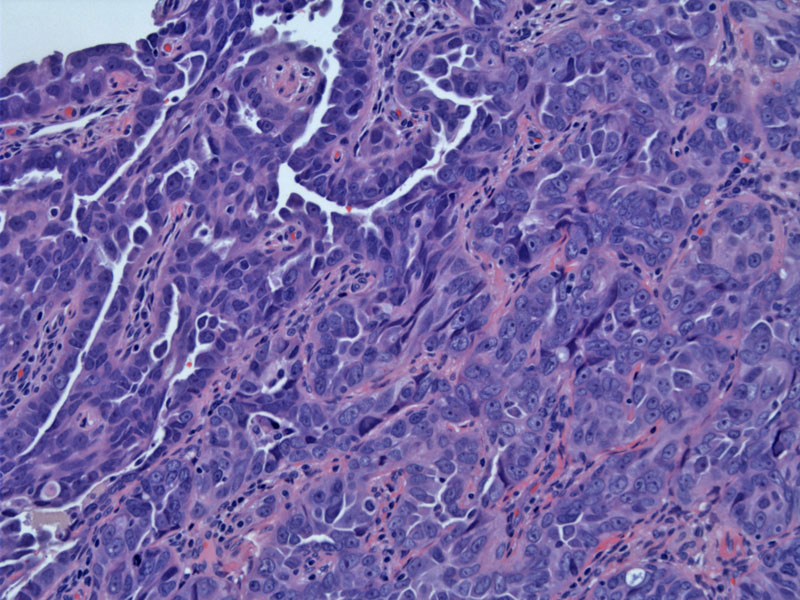
Papillae are lined by malignant serous cells admixed with areas of solid growth. The histology is identical to that seen in the ovary.
){kind=link}
At higher magnification, prominent nuclear atypia can be appreciated.
){kind=link}
Several years later a subcutaneous nodule appeared in the abdominal area. The corresponding cytology (Thin prep) reveals a cluster of malignant cells with pleomorphic nuclei and prominent nucleoli indicative of recurrent adenocarcinoma.
){kind=link}
At low power, the same malignant cells are seen in the cell block.
){kind=link}
At higher power, the nuclear pleomorphism is evident.
){kind=link}
Bizarre nuclei, small cytoplasmic vacuoles and prominent nucleoli are characteristic features.
){kind=link}
Traditionally, neoplasms in the fallopian tube were thought to arise via three distinct pathways: (1) metastases from the ovary or endometrium; (2) arising from foci of endometriosis; (3) primary tumors of the fallopian tube. The last pathway is the least common, as primary tubal carcinomas are rare and account for less than 1% of female genital tract malignancies.1
The majority of primary ovary carcinoma (1/2 to 2/3 depending on the study) are of the serous type. The second most common type is endometrioid, followed by transitional cell and undifferentiated carcinoma. Interestingly, mucinous and clear cell carcinomas are exceedingly rare in the fallopian tube.
Since serous carcinoma of the ovary is virtually identical histologically to serous carcinoma of the fallopian tube and far more common, to diagnose a primary tubal carcinoma, the following criteria should be strictly applied: (1) the majority of the tumor resides in the fallopian tube; (2) the ovary and uterus should either be normal or contain less tumor than the fallopian tube; (3) transition from normal to malignant epithelium (ie. intraepithelial carcinoma) seen within the tube.
Recent studies of familial breast-ovarian syndromes have revealed that primary tubal tumors are more common in patients with BRCA1 or BRCA2 mutations. Thus, if undergoing prophylactic gonadectomy to decrease cancer risk, these patients should have their fallopian tubes as well as their ovaries removed.
The incidence of primary malignant tumor of the fallopian tube is reported to be below 1%, however, its true incidence may be underestimated as advanced tumors that have spread to the ovary are usually diagnosed as primary ovarian tumors.
Tubal caricinomas affect middle-aged women (average age is 55), but can occur over a wide age range (age 20 to 80). The finding of profuse watery vaginal discharge in a postmenopausal woman is virtually pathognomic for this malignancy. Most patients present with carcinomatosis- a condition where the peritoneal cavity fills with malignant ascites and most peritoneal surfaces have malignant implants. Patients experience increasing abdominal girth, fullness, pain, and typically a pelvic mass can be palpated on exam.
15% of patients with tubal carcinoma have BRCA1 or BRCA2 mutations. Pre-treatment CA-125 levels correlate with tumor stage and similar to ovarian carcinomas, CA-125 can be used to monitor disease progression or response to treatment.2
Complete surgical staging involving hysterectomy with bilateral salpingo-oophorectomy, pelvic and peritoneal biopsies, washings, pelvic lymphadenectomy, and omentectomy is performed. At the time of staging, a goal of optimal cytoreduction (no residual disease >1cm) is attempted. Staging procedures are followed with a platinum based chemotherapy regimen.
Poor prognostic factors include deep invasion into the tubal wall, tubual rupture and location at the fimbriae (versus location in the ampulla or isthmus). The most important prognostic factor, however, is stage. In one study, survival rates for stage I, III, III and IV tumors were 95%, 75%, 69% and 45% respectively.2 While most patients do eventually reach a level of remission, recurrence rates are very high.
• Endometrium : Papillary Serous Adenocarcinoma
• Ovary : Serous Adenocarcinoma, High Grade Papillary
1 Crum CP, Lee KR. Diagnostic Gynecologic and Obstetric Pathology. Philadelphia, PA: Elsevier; 2006: 697-706.
2 Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 625-7.