
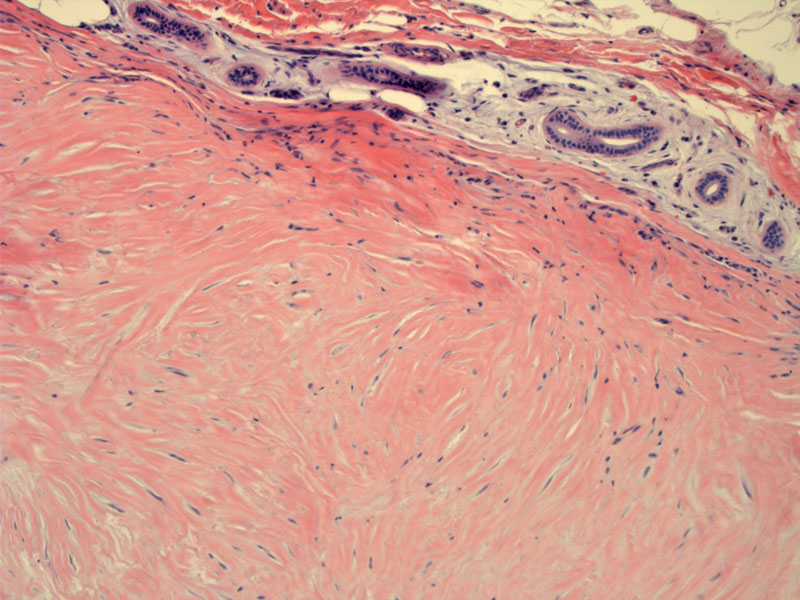
The lesion shows a densely collagenized rim, which compressed but does not infiltrate the overlying normal adnexal structures; the lesion arises in the immediate superficial dermis.
){kind=link}
Similarly, its deep border is expansile and not infiltrative. This is one useful feature to distinguish it from more aggressive mesenchymal vulvar lesions.
){kind=link}
Much of the lesion shows a myxohyalinized stroma and scattered small delicate spindled nuclei. Image
){kind=link}
Alternating areas of collagen with intervening myxoid stroma are seen and some curvilinear thin-walled vessels. Thick-walled vessels, typical of aggressive angiomyxoma, are not a feature of this lesion.
){kind=link}
The actual cells are extremely tapered and the myxoid nature of the cytoplasm can be appreciated.
){kind=link}
Some areas are more densely collagenized with wavy eosinophilic bands in different directions, and a few multinucleated cells are observed.
){kind=link}
These lesions are usually negative for ER. The PR in this case was also negative. ER/PR negativity is yet another feature distinguishing it from aggressive angiomyxoma, which are often ER/PR positive.
){kind=link}
CD34 stains the myxoid cells, illustrating the elongate cytoplasm.
){kind=link}
Smooth muscle actin (SMA) stains the cells in this area; other areas were negative. Desmin staining is negative.
){kind=link}
Superficial angiomyxomas are most commonly encountered in the head and neck region and the trunk, and occasionally, it is found in the genital regions of both men and women. When multiple angiomyxomas arise in other sites, they may be a feature of Carney's syndrome, however, angiomyxomas in the vulvovaginal region do not have a clear association with this complex.1
Microscopically, this neoplasm is non-encapsulated, but well-demarcated. It is nodular myxoid proliferation that is located in the superficial dermis. The mxyoid nodules are comprised of delicate spindled cells with thin-walled vessels. Scattered inflammatory cells, especially neutrophils, are commonly found.
It is important to distinguish this lesion from deep (aggressive) angiomyxoma as deep angiomyxomas are infiltrative, locally destructive with a strong propensity to recur after excision. Superfical angiomxyomas recur as well, however, they are not locally destructive.
In unclear situations, IHC will be helpful. In an AFIP study of 17 cases of superficial angiomxyomas, the tumors were immunoreactive for vimentin (11/11), CD34 (11/11), muscle-specific actin (8/12), smooth muscle actin (9/11), S100 protein (5/13), and Factor XIIIa (5/9). No immunoreactivity was present for desmin (DE-R- 11), glial fibrillary acidic protein, estrogen receptor or progesterone receptor. In contrast, deep angiomyxomas are immunoreactive for ER, PR and desmin.2
Similar to deep (aggressive) angiomyxomas, they arise most commonly in the 4th decade and presents as a painless, slowly growing polypoid mass. These lesions usually measure less than 5 cm (whereas deep angiomyxomas are often larger than 10 cm). Due to their high myxoid content, they exhibit a gelatinous cut surface.3
Excision with a small rim of normal tissue if possible.
Benign; do not metastasize, but local non-destructive recurrence occurs in 30% of cases.
• Vulva : Cellular Angiofibroma
• Vulva : Angiomyofibroblastoma
• Vulva : Deep (Aggressive) Angiomyxoma
1 Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 742-3.
2 Fetsch JF, Laskin WB, Tavassoli FA. Superficial angiomyxoma (cutaneous myxoma): a clinicopathologic study of 17 cases arising in the genital region.
Int J Gynecol Pathol 1997 Oct;16(4):325-34.
3 Nucci MR, Oliva Esther. Gynecologic Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier: 2009: 37-8.