
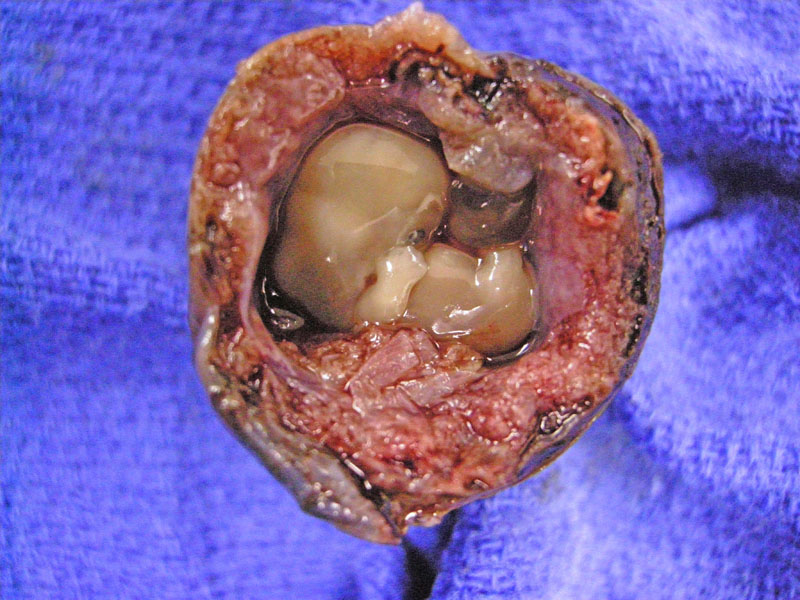
A cross section of a fallopian tube with a fetus.
){kind=link}
Tubal pregnancy is the most common cause of hematosalpinx (blood in the tube) and should always be suspected if one finds a hematoma within the tube. The placental tissue often invades through the tubal wall, leading to rupture and intraperitoneal hemorrhage.
){kind=link}
Trophoblastic proliferation extending into the outer wall of the fallopian tube (seen on the upper left).
){kind=link}
Tubal epithelium arranged in plicae is seen here against a background of trophoblasts and dissecting hemorrhage.
){kind=link}
Chorionic villi can be appreciated here.
){kind=link}
Ectopic pregnancy refers to implantation of the fetus at any location other than the uterus. The most common site (90%) occur in the ampulla or isthmus of the fallopian tube. Other sites include the cornu (intrauterine portion of the fallopian tube), ovary and abdominal cavity.
Ectopic pregnancies occur in approximately 1 in 150 pregnancies. The most significant risk factor is a history of pelvic inflammatory disease with salpingitis. Other predisposing conditions include peritubal adhesions from previous surgeries and endometriosis. 50% of ectopic pregnancies occur in normal appearing tubes, however.1
Abdominal pregnancies occur when the fertilized ovum falls out the fimbriated end of the fallopian tube and implants in the abdominal cavity. Exceptionally, the fetus may continue to full term and be delivered surgically. In even rarer instances, the fetus dies and becomes calcified, turning into a lithopedion (lithos - stone; paidion - child).2
The classic presentation is a reproductive age woman with severe abdominal pain, peritoneal signs, a menstrual period 6-8 weeks prior, and a positive pregnancy test. The pain may mimic appendicitis if the pregnancy is in the right fallopian tube. In cases of tubal rupture, early diagnosis and immediate surgery will save her life.
More often nowadays patients will present in the first trimester of pregnancy with vaginal spotting with or without pelvic cramping. Subsequent ultrasound evaluation will fail to demonstrate a pregnancy inside the uterus despite a human chorionic gonadotropin level above 2000 (a level at which most pregnancies should be seen ultrasonographically).
An endometrial biospy may demonstrate decidual changes in 50% of instances, but unless the very rare heterotopic pregnancy (one in the tube and one in the uterus) occurs, chorionic villi will not be found in the biopsy.
Ectopic pregnancies may be treated medically with methotrexate in the stable, nonruptured patient with no contraindications to methotrexate. Earlier gestations are more likely to be successfully treated medically. For surgical management, patients may have the ectopic removed via a salpingostomy or a salpingectomy.
Many patients with a history of an ectopic pregnancy will go on to have a normal pregnancy in their future. However, as fallopian tube conditions appear to predispose patients to ectopic pregnancies the patient will be at higher risk of recurrence. If a salpingectomy is performed to treat the ectopic pregnancy, the abnormal tube will be absent. However there is no guarantee the noninvolved fallopian tube will be normal. Additionally, decreased fertility rates have been observed in women who have undergone salpingectomy to treat an ectopic pregnancy.
1 Kumar V, Abbas AK, Fausto N. Robbins and Cotran Pathologic Basis of Disease. 7th Ed. Philadelphia, PA: Elsevier; 2005: 1105.
2 Moore KL, Persaud TVN. The Developing Human: Clinically Oriented Embryology. 7th Ed. Philadelphia, PA: Saunders: 2003; 47-8.