
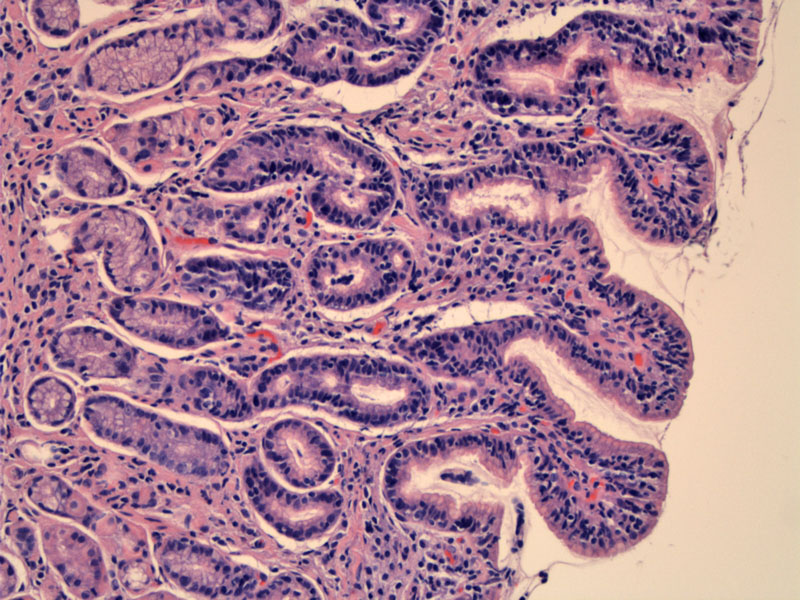
Villous transformation of the antrum is seen along with increased cellularity within the surface epithelium appreciated.
){kind=link}
The foveolar epithelium is mucin depleted and involved by a heavy number of intraepithelial lymphocytes.
){kind=link}
prominent villi seen here with excessive lymphocytes obscuring the epithelial nuclei.
){kind=link}
A similar process is seen in the gastric body, but it seems like the oxyntic area underneath with the parietal cells is relatively spared. The lamina propria contains lymphocytes but not an overwhelming number.
){kind=link}
The glands are separated by a dense lamina propria lymphocytic infiltrate.
){kind=link}
A different area in the body has some acute inflammation and glandular damage. The arrow shows a gland attacked by neutrophils.
){kind=link}
a fragment of fibrinopurulent debris was also in this specimen, indicative of an area of ulceration.
){kind=link}
The normal number of intraepithelial T lymphocytes in the stomach is 1 or less per 100 epithelial cells. An increase in the number of gastric intraepithelial lymphocytes (IELs) can occur as a reactive process such as due to Helicobacter pylori infection, celiac sprue, Ménétrier disease, and Crohn disease or as an indiopathic condition (Carmack). The latter is termed "lymphocytic gastritis" and is diagnosed when the gastric surface and foveolar epithelium is infiltrated by at least 25 IELs per 100 epithelial cells, regardless of the inflammation in the lamina propria. The IELs are CD8 positive. It is associated with celiac disease and in such cases, the increased IELs are largely antral in distribution.
There is a variant of lymphocytic gastritis termed hypertrophic lymphocytic gastritis, in which patients present with dyspepsia and protein loss (lower extremity edema, hypoalbuminemia) and endoscopy shows giant gastric folds. Histology resembles Ménétrier disease with the additional finding of prominent IELs (Charton-Bain)
Adults and children may be affected. Initially it was thought that most patients present with symptoms, including dyspepsia, nausea, vomiting, and weight loss. Subsequently, a significant percentage of patients have presented with only mild nonspecific dyspeptic symptoms and a normal endoscopic appearance of the stomach.
Endoscopically, the characteristic appearance included large folds, varioliform (“octopus-sucker”) gastritis, nodules, and erosions was often present.(Carmack)
Treatment focuses on the underlying condition if there is one, such as celiac disease. If ulcers are present, a proton pump inhibitor may be employed.
Benign.
Carmack SW, Lash RH, Gulizia JM, Genta RM. Lymphocytic disorders of the gastrointestinal tract: a review for the practicing pathologist. Adv Anat Pathol. 2009 Sep;16(5):290-306.
Charton-Bain MC, Paraf F, Bruneval P. Superficial gastric carcinoma developed on localized hypertrophic lymphocytic gastritis: a variant of localized Menetrier's disease? Pathol Res Pract. 2000;196:125–128.