
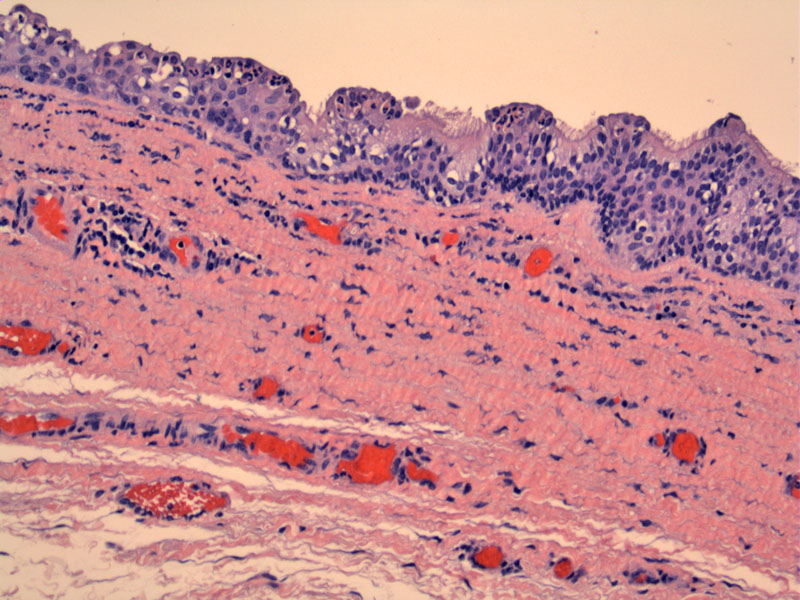
A typical multilayered lining is seen in this vaginal cyst. Ciliated cells are seen in the superficial surface as well as acute inflammatory cells. Note the elastic fibers and congested blood vessels in the vaginal wall.
){kind=link}
Metaplastic squamous epithelium is seen lining this cyst. More mature squamous epithelium is seen on the left. We will not attempt to subclassify these cysts into paramesonephric, mesonephric or squamous cysts. Simply note that the cysts can be lined by a variety of epithelia.
){kind=link}
A simpler lining with ciliated columnar cells can be appreciated here. Note the presence of numerous neutrophils.
){kind=link}
Squamous epithelium (likely metaplastic) is seen on left while ciliated columnar epithelium is seen on right.
){kind=link}
This case demonstrates a more attenuated lining with inflammation in the underling stroma.
){kind=link}
Vaginal cysts can be broadly divided into four main categories: paramesonephric (Mullerian) cysts, mesonephric (Wolffian) cysts, traumatic (squamous) cysts or urogenital cysts (Bartholin gland cysts). The first two entities are most commonly found in the upper vagina while the latter two are usually located in the distal vagina.1
(1) Paramesonephric cysts: The most common type of vaginal cysts, paramesonephric cysts are lined by Mullerian-type epithelia (endocervical, endometrial, tubal or mucinous epithelium). Some arise in DES-exposed patients with vaginal adenosis.2
(2) Mesonephric cysts: The most well-known entity in this category is the Gartner's duct cyst. They are considered to be of mostly of mesonephric (Wolffian) duct origin and lined by cuboidal to columnar epithelium. However, many Gartner's cysts are now believed to be also derived from paramesonephric ducts and thus, may be lined with Mullerian-type epithelia as well.2 Gartner's duct cysts develop when fluid collects in Gartner's duct, a vestigial structure left over from embryonic development. These cysts are usually located in the side walls of the upper vagina.
(3) Epithelial inclusion (squamous) cysts: Lined by squamous epithelium, these cysts generally occur as a result of trauma (ie. episiotomy or lacerations). The cysts may be filled with keratin and sebaceous material.
(4) Urothelial-lined cysts: Bartholin's glands are formed by a ductal structure lined by transitional epithelium and surrounding clusters of mucinous acini. When the secretions become blocked, a cyst may form.
Most cysts are asymptomatic. However, the cyst may enlarge from blocked secretions or infection, thus, bringing it to attention. The cysts may cause discomfort and dyspareunia.
Distinguishing between mesonephric, paramesonephric and squamous cysts is largely an academic exercise. Often, they cannot be categorized with certainty -- this is not concerning since clinically, they are benign and treated conservatively.
• Vulva : Bartholin Gland Cyst
• Fallopian Tube : Paratubal Cyst
1 Robboy SJ, Anderson MC, Russell P. Pathology of the Female Reproductive Tract. London, UK: Churchill Livingstone; 2002: 80-1.
2 Crum CP, Lee KR. Diagnostic Gynecologic and Obstetric Pathology. Philadelphia, PA: Elsevier; 2006: 234-5.