
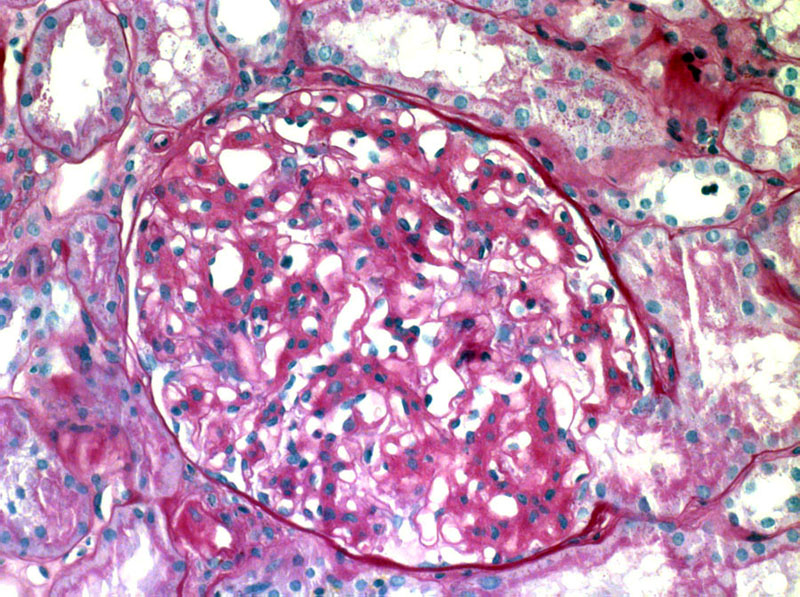
The glomeruls is relatively intact, although affected by a discernable increase in mesangium.
){kind=link}
The fibrils usually stain for Ig) and C3. In this image, IgG is present along capillary walls and within the mesangium. Some cases have IgM and/or IgA as well.
){kind=link}
Some reactivity for C3 is often present as well.
){kind=link}
The EM shows a widened paramesangium. A granular appearance is appreciated at this power.
){kind=link}
EM shows randomly arranged, nonbranching fibrils that measure 12 to 24 nm in diameter. This contrasts with the fibril size in amyloid-- usually between 8 and 15 nm.
){kind=link}
A different case shows a striking pattern of amorphous acellular material which appears to infiltrate mesangial regions and peripheral cappilary walls. It is unaccompanied by any significant cellular proliferation.
){kind=link}
Part of this glomerulus is more affected than the other, with the bottom right affected by heavier deposits obscuring the architecture resulting in the appearance of
){kind=link}
Some glomeruli are afflicted by crescentic injury along with a few neutrophils. Crescents affect about 1/3 of all cases reported.
){kind=link}
The kidney also shows chronic interstitial damage with some fibrosis separating the tubules, and thickened wrinkled tubular basement membranes.
){kind=link}
Another image again shows tubular atrophy which is chronic.
){kind=link}
Chronicity is also appreciated in the form of the early onset of periglomerular fibrosis.
){kind=link}
Organized fibrillar or microtubular glomerular deposits are encountered in a variety of renal disorders-- amyloidosis, cryoglobulinemic glomerulonephritis, lupus nephritis, collagen glomerulopathies, and the rare entities of fibrillary and immunotactoid glomerulonephritis. Fibrillary glomerulonephritis (FGN) designates a renal condition characterized by glomerular accumulations of nonbranching, randomly arranged fibrils that are ultrastructurally indistinguishable from amyloid fibrils. Importantly, the fibers differ from amyloid by their larger size and lack of reactivity with Congo Red.
Diagnosis requires electron microscopic identification of these infiltrating fibrils within the glomerulus.
The histologic appearance is diverse, with the more common patterns including a membranoproliferative glomerulopathy, diffuse proliferative glomerulonephritis,and mesangial proliferative glomerulopathy.
FGN affects a wide age range (rarely the pediatric population) and has most frequently been described in middle-aged to older patients. Individuals have proteinuria,and about half experience nephrotic range proteinuria. Hematuria and hypertension are not uncommonly encountered.
Immunosuppressive therapy is often employed.
Most patients have a poor outcome despite immunosuppressive therapy. Some patients do show a transient partial response to this treatment. One study confirmed the high risk of end-stage renal disease, with a median renal survival of only 24 months from the time of biopsy (Rosenstock). Patients with the diffuse sclerosing pattern or severe proliferative pattern had a worse outcome in this study.
FGN is an idiopathic condition resulting from polyclonal immune deposits
Fibrils usually stain for IgG and C3
Despite immunosuppressive agents, ESRD is common
Rosenstock JL, et al. Fibrillary and immunotactoid glomerulonephritis: Distinct entities with different clinical and pathologic features. Kidney Int. 2003 Apr;63(4):1450-61.