
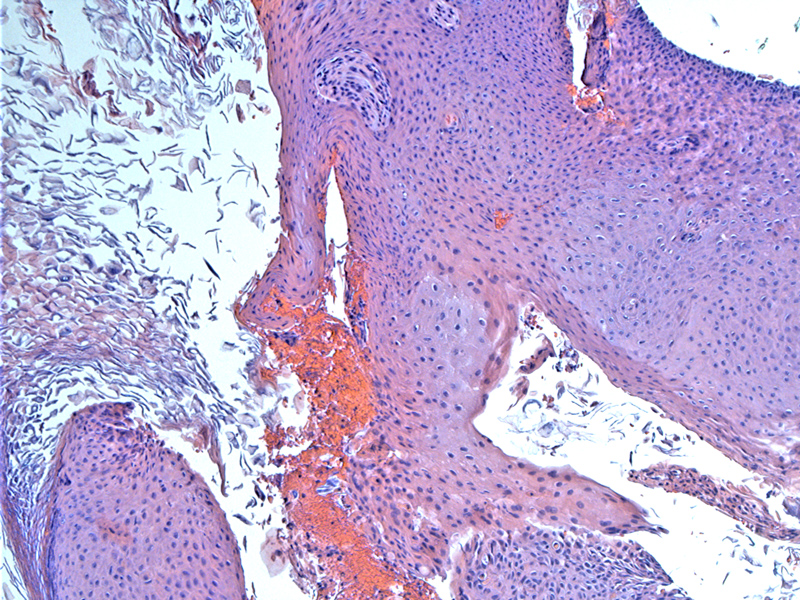
Mature multilayered squamous epithelium with marked keratin production. Occasionally, cholesterol crystals (for which the lesion was named) can be seen. This particular case did not contain any cholesterol clefts.
){kind=link}
Note the desquamating layers of keratinized epithelium.
){kind=link}
Neutrophils are congregating in the lesion -- sometimes Pseudomonas infects the debris.
){kind=link}
Cholesteatoma is a cystic lesion located in the middle ear derived from keratinizing stratified squamous epithelium. The resulting hyperkeratosis and shedding of keratin debris results in a cystic mass which often incites an inflammatory reaction. It can be congenital or acquired. Congenital lesions occur when squamous epithelium becomes trapped in the temporal bone during embryogenesis. Acquired cholesteomas occur after injury to the tympanic membrane, either from perforation or infection.1,2
Congenital cholesteomas present at an earlier age (5 months to 5 years of age) whereas acquired cholesteatomas usually occur in older individuals, with a history of chronic ear infections or trauma to the ear. Common symptoms include otorrhea (serous or purulent discharge), dizziness and conductive hearing loss. Often, a white retrotympanic middle ear mass can be visualized.2
Complete surgical excision is required. Besause there is no blood supply to the cholesteoma, antibiotics are not effective. If not removed, growth of cholesteaomas can destroy surrounding bone. The pressure of the growing squamous lesion will elict bone remodeling and furthermore, osteolytic enzymes are active in the periphery of the lesion, leading to bone resorption.
Depending on the location of the lesion and the surgery technique employed, the risk of recurrence ranges from 5 to 40%. Usually, the lesion stays within the confines of the temporal bone, but occasionally may extend into the neck and brain and in rare cases, cause neurologic dysfunction from a mass effect.2
1 Semaan MT, Megerian CA. The pathophysiology of cholesteatoma. Otolaryngol Clin North Am. 2006 Dec;39(6):1143-59.
2
Roland PS. Middle ear Cholesteoma: eMedicine. Last updated on June 2009. Available at: http://emedicine.medscape.com/article/860080-overview