
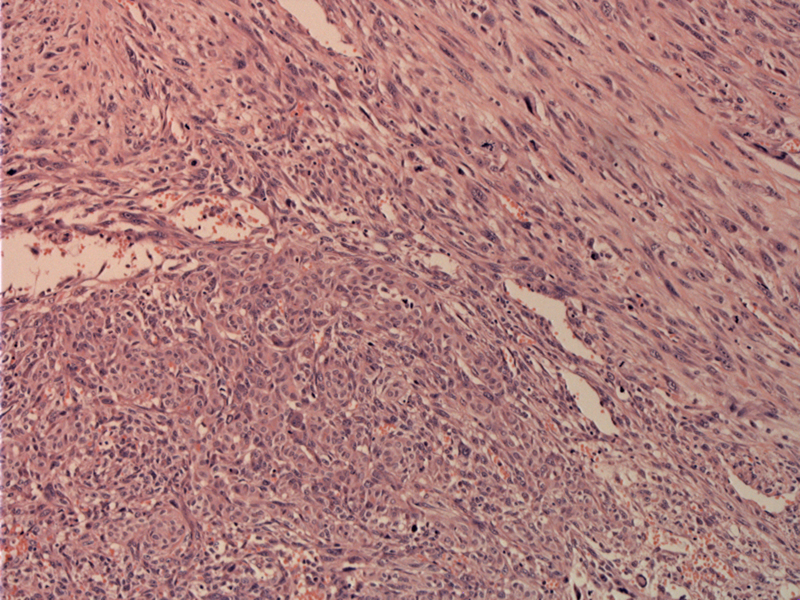
This is a highly cellular neoplasm with fascicles of spindle cells growing in various planes.
){kind=link}
Atypical nuclei are easy to find.
){kind=link}
Numerous mitotic figures can be appreciated in this area of plump spindle cells.
){kind=link}
Fascicular bundles of spindle cells lend a sarcomatous look to the tumor.
){kind=link}
Undifferentiated (anaplastic) carcinoma can arise de novo, or from a pre-existing well-differentiated thyroid carcinoma. It is an aggressive stage T4 tumor that affects the elderly.
Grossly, the cut surface is fleshy, tan-white surface with frequent areas of necrosis and hemorrhage. Histologically, a combination of spindle cell, pleomorphic giant cell and epithelioid cells form fascicles or solid sheets. Often, a single cell type may predominate. For example, a predominantly spindle cell type may resemble a sarcoma.
Mitotic activity, coagulative necrosis, intensive neutrophilic infiltration, effacement of blood vessels by tumor are all common features. A thoroughly sampled mass will often demonstrate areas of well-differentiated carcinoma, supporting the theory that undifferentiated thyroid carcinoma is a result of dedifferentiation (DeLellis).
Because of dedifferentiation, TTF-1 and thyroglobulin immunostains are rarely positive. Keratin, EMA, vimentin will be positive in most cases. p53 mutations are common and thus, most cells will stain for this marker (Thompson).
Of note, poorly-differentiated (insular) carcinoma is thought to lie between well-differentiated and undifferentiated carcinoma in terms of morphology and behavior; however, poorly-differentiated carcinoma is currently a controversial entity. The key differences between the two include the absence of prominent nuclear pleomorphism and mitotic activity, abortive follicle formation and thyroglobulin reactivity seen in poorly-differentiated carcinomas (DeLellis, Fletcher). Yes, the terminology is terrible (poorly-differentiated versus undifferentiated), but hey, I didn't make the rules.
There is extensive replacement of normal thyroid and invasion into surrounding structures such as the larynx, trachea and pharynx, resulting in a fixed and firm mass. Slightly more common in females (F:M ratio of 1.5:1), and usually seen in older patients (mean age of 70). The presentation is that of a rapidly enlarging mass, leading to hoarseness and dysphagia. As this is an aggressive tumor, regional or distant metastasis (usually lungs and bones) may be detected. Rarely, the tumor may elaborate G-CSF and cause leukocytosis.
With iodine supplementation, the incidence has decreased substantially. Previous radiation is also another risk factor (Fletcher).
The tumor is usually widely metastatic and inoperable. Chemotherapy has met limited success.
Dismal. The median survival rate is less than 4 months (Fletcher).
• Thyroid : Anaplastic Carcinoma, Pleomorphic Giant Cell Type
• Thyroid : Anaplastic Carcinoma, with Osteoclast-like Giant Cells
• Thyroid : Anaplastic Carcinoma, Squamoid Type
DeLellis RA, Lloyd RV, Heitz PU, Eng C. Tumors of Endocrine Organs: WHO Classification of Tumours. Lyon; IARC Press; 2004: 77-80.
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: .
Thompson LDR. Endocrine Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier; 2006: 109-113.