
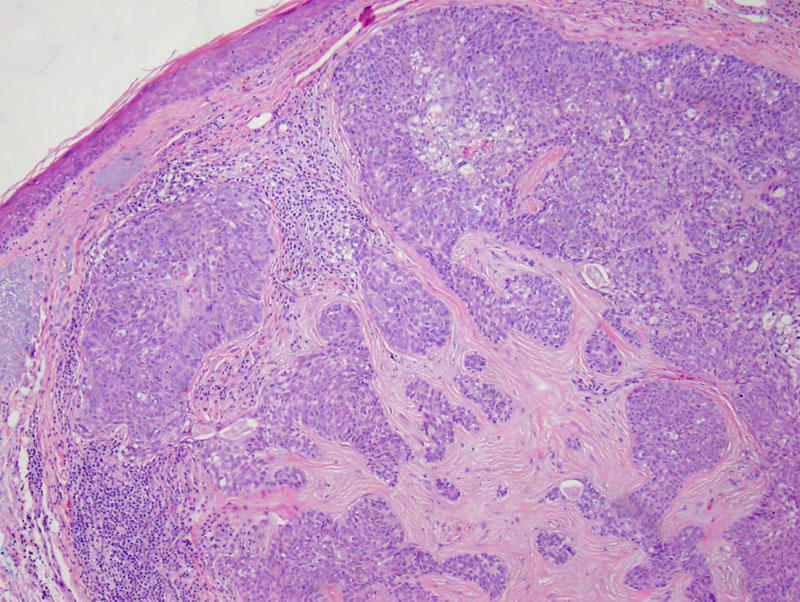
Case 1: Nests and cords of neoplastic cells dissect through the dermal stromal tissues.
Note that the prominence of pleomorphic basaloid cells with scattered sebocytes. These malignant cells are pleomorphic and mitotically active.
Lobules of malignant cells are present within the collagenous stroma along with some lymphocytes.
Variable cell size and shape can be appreciated here as well as a different quality to the cytoplasm.
The neoplastic sebaceous cells are immunoreactive for EMA.
Positivity for keratin 7 is demonstrated here.
Sebaceous carcinoma may be associated with the very rare Muir–Torre syndrome, a cancer syndrome associated with a defect in a DNA mismatch repair gene. Criteria for the diagnosis of Muir-Torre syndrome include at least one sebaceous adenoma, sebaceous epithelioma, or sebaceous carcinoma, and at least one visceral cancer.
Sebaceous carcinomas are categorized as either periocular or extraocular. The distinction is important, as malignant sebaceous tumors are more likely to arise in the periocular region. Extraocular tumors are rare in sporadic cases, but are more common in patients with Muir-Torre syndrome (Busam, Fletcher). These tumors represent the second or third most common eyelid malignancies after basal cell carcinoma (and squamous cell carcinoma.).
Histologically, a nodular growth pattern with invasion into the surrounding stroma is seen. In sebaceous adenomas, sebocytes predominate whereas in sebaceous carcinomas, the dominant population shifts to the basaloid cells. The basaloid cells and sebocytes are atypical and mitotically active. Depending on the number of mature sebocytes, the lesion is categorized as well, moderately or poorly differentiated lesions. In poorly differentiated tumors, basaloid cells may appear spindled and sarcomatoid with sparsely scattered sebocytes (Busam).
Pagetoid spread may be seen in sebaceous carcinoma and should be distinguished from extramammary Paget disease. IHC will be helpful as extrmammary Pagets is CEA+ and mucin+ and these markers are negative in sebaceous carcinoma (Busam).
Typically occurs in older individuals. A yellow-red, sometimes ulcerated lesion is seen. Areas rich in sebaceous glands are most affected such as eyelid, head and neck. Most often found in the periocular area as a painless subcutaneous nodule. Periocular sebaceous carcinoma may sometimes be thought clinically to be an inflammatory condition such as chalazion or blepharoconjuntivitis.
Excision is required. In a review of patients with 5- to 6-mm excision margins , the 5-year mortality rate of 18% and recurrence rates of up to 36% at 5 years (Shields). Although thought to be resistant to radiation, isolated case reports have shown remission with treatment (Conill).
These tumors are aggressive, with high rates of recurrence and metastasis. Mortality ranges from 9% to 50%.
→Sebaceous carcinoma may be associated with Muir–Torre syndrome, a cancer syndrome related to a defect in a DNA mismatch repair gene.
→Sebaceous carcinoma most frequently affects the eyelid; they arise from modified sebaceous glands (Meibomian glands).
Basam KJ. Dermatopathology: Foundations in Diagnostic Pathology 1st Ed. Philadelphia, PA: Elsevier; 2010: 431-4.
Conill C et al. Radiation therapy as a curative treatment in extraocular sebaceous carcinoma, Br J Dermatol 149 (2003), pp. 441–442.
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 1451-2.
Shields JA et al. Sebaceous carcinoma of the ocular region: a review, Surv Ophthalmol 50 (2005), pp. 103–122.

){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}