
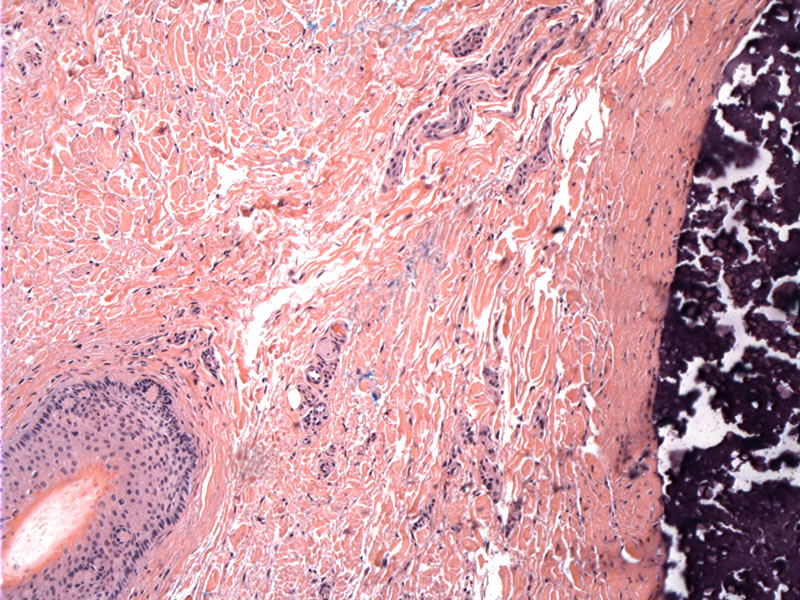
An adnexal structure is seen in the lower right for orientation. The right side shows the densely staining basophilic calcium deposits surrounded by a fibrous capsule.
){kind=link}
High power image showing dense deposits of calcium.
){kind=link}
This additional case is one of idiopathic scrotal calcinosis. A low power view nicely demonstrates the superficial scrotal epithelium with a nodule of calcium deposits in the dermis.
){kind=link}
Calcinosis cutis is a term used to encompass a broad range of entities that share the common feature of calcium deposition in cutaneous tissue. It is generally classified into four major types: dystrophic, metastatic, iatrogenic and idiopathic (Rapini, Walsh).
Dystrophic calcification is the most common form and thought to arise as the result of a local inflammatory process, leading to secondary calcium deposition in soft tissue. Causes of dystrophic calcification include connective tissue disease (e.g. scleroderma and CREST), panniculitis (pancreatic enzyme panniculitis), hereditary conditions (pseudoxanthoma elasticum, Ehlers-Danlos, porphyria cutanea tarda), cutaneous tumors (pilomatricoma, pilar cysts, basal cell carcinoma, chondroid syringomas), and infections (onchocerciasis, cysticercosis).
Metastatic calcification is often the result of an underlying defect in calcium and/or phosphate regulation such as hyperparathyroidism that may be primary or secondary from renal failure. Other causes include hypervitaminosis D and milk-alkali syndrome.
A common example of idiopathic calcification is "calcinosis scroti", a condition in which multiple calcified nodules arise within the wall of the scrotum. Approximately 123 cases have been reported in the literature according to a review done by Saladi et al in 2004. The nodules are slow growing and age of onset is about the 3rd decade. Histologically, deposits of calcium and keratin flakes are encased in a fibrous capsule with sparse inflammation +/- an epithelial lining. Proposed etiologies include calcification of eccrine or epidermal inclusion cysts within the scrotum, dystrophic calcification in the smooth dartos muscle and truly idiopathi (Saladi, Weedon).
The clinical presentation can vary widely from a solitary, small, firm, dermal nodule to a more diffuse process with multiple cutaneous nodules.
Treatment varies depending on the underlying process. Surgical excision may be used to treat individual nodules. There is no uniform method for the treatment of dystrophic calcification, but therapies include a low calcium and phosphate diet and diltiazem. The underlying etiology causing calcinosis in patients with metastatic calcification must be identified and treated appropriately.
Bolognia JL, Jorizzo JL, Rapini RP, eds. Dermatology. 2nd ed. St. Louis, MO: Mosby; 2008.
Saladi RN, et al. Scrotal calcinosis: is the cause still unknown? J Am Acad Dermatol. 2004 Aug;51(2 Suppl):S97-S101.
Walsh JS, Fairley JA: Calcifying disorders of the skin. J Am Acad Dermatol. 1995;33:693-706.
Weedon D. Weedon’s Skin Pathology. 3rd ed. Philadelphia, PA: Elvsevier; 2010:370-2.