
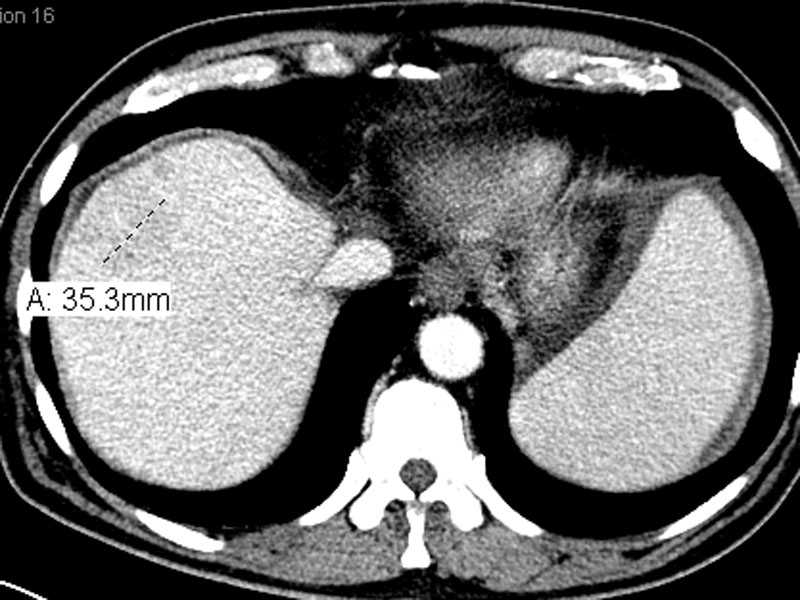
CT scan shows an ill-defined mass centered on liver segments 4a and 4b.
){kind=link}
Case 1 - Neoplastic epithelial cell proliferate in a cribriform pattern.
){kind=link}
Jagged glands dissect into a heavily desmoplastic stroma. A cribriform gland is noted.
){kind=link}
In some areas, cords and trabeculae are formed.
){kind=link}
The cells have round nuclei with light pink or vacuolated cytoplasm. Nucleoli are seen but are not especially prominent.
){kind=link}
Case 2 - Intraductal high grade dysplasia are seen in the glands.
){kind=link}
The neoplastic cells contained abundant mucin (mucinous variant). Note the marked pleomorphism.
){kind=link}
Case 3 - This tumor was composed of small tubular glands in a highly sclerotic background.
){kind=link}
Mucicarmine stains the mucin pink. This is a helpful stain in differentiating cholaniogcarcinoma (an adenocarcinoma) from hepatocellular carcinoma, which does not produce mucin.
){kind=link}
Case 4 - This tumor illustrates an almost back-to-back proliferation of ductal or tubular structures embedded in a densely sclerotic stroma.
){kind=link}
At higher power, nuclear pleomorphism and heterogeneity of the cells within the same irregular jagged ducts can be appreciated.
){kind=link}
Cholangiocarcinoma are malignant tumors arising from bile ducts and are broadly divided into intrahepatic and extrahepatic (perihilar) locations. The incidence appears to be arising despite accounting for greater detection of the tumor. The reason for this is unknown (Fletcher, Iacobuzio). In the US, 20-30% are intrahepatic while the rest arise in an extrahepatic location (Fletcher).
Predisposing conditions include chronic inflammation of the bile ducts such as primary sclerosing cholangitis, infections by bacteria and liver flukes (i.e. Clonorchis sinesis, Opisthorchis viverrini, parasites endemic in the Far East), and Thorotrast administration (radioactive contrast medi banned in the 1950s, but associated risk lasts for many decades). Cholangiocarcinoma can also arise in the setting of HNPCC (hereditary non-polyposis colon cancer)(Fletcher).
Grossly, intrahepatic cholangiocarcinoma is white-tan mass with infiltrative or well-circumscribed borders. Due to a robust desmoplastic response, the tumor is firm and gritty areas represent dystrophic calcifications. The normal liver is usually non-cirrhotic.
Over 95% of cholangiocarcinoma are adenocarcinomas. Histologically, columnar or cuboidal tumor cells with clear or pink cytoplasm form tubular glands and ducts. Like other pancreatic-biliary carcinomas, an interesting feature is the heterogeneity of the glandular cells within the same neoplastic gland (Rosai). Intracellular mucin production can be highlight with special stains. There is usually a prominent desmoplastic stroma. Perineural and perivascular invasion are common.
Less common microscopic variants include mucinous, signet ring, adenosquamous, sarcomatous, small cell and EBV-associated lymphoepithelioma-like carcinoma.
The main differential diagnosis is hepatocellular carcinoma and metastatic adenocarcinoma. Hepatocellular carcinoma tends to exhibit different morphology, with trabecular or acinar architecture and scant fibrous stroma (caveat: sclerosing variant of HCC) and patients often have elevated AFP. Cholangiocarcinomas will stain positively with mucicarmine, whereas mucin is usually absent in HCC. Hepatocellular carcinoma is also HepPar1, AFP and polyclonal CEA (canalicular pattern), albumin ISH positive and nonreactive with monoclonal CEA, CK19 and MOC31. Cholangiocarcinoma is positive for MOC31, CK19 and polypclonal CEA (cytoplasmic pattern) and negative for HepPar1 and AFP (Fletcher).
Metastatic adenocarcinoma (i.e. from pancreas, breast, lung, GI tract) can be difficult to distinguish from primary cholangiocarcinoma. CK7 and CK20 can be helpful in a subset of cases since colorectal adenocarcinomas are usually CK7-/CK20+ whereas intrahepatic cholangiocarcinomas are CK7+/CK20+. Extrahepatic cholangiocarcinomas, however, are CK7+/CK20+ (Fletcher, Rosai).
Predominantly affects adults (between 50-70 years) with equal gender distribution. Patients present with abdominal pain, anorexia and weight loss. In some cases, the tumor can remain asymptomatic until it reaches an advanced stage. Elevated CA19-9 suggests malignancy, but it is nonspecific and also seen in primary sclerosing cholangitis as well as carcinomas of the stomach and pancreas.
Survival is highly dependent on the resectability of the tumor and tumor stage. Tumor grade has very little bearing. Those with resectable tumors have survival of up to 30 months. Those with unresectable tumors (unfortunately, the majority of cases) have a survival of less than 6 months.
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 451-453.
Iacobuzio-Donahue CA, Montgomery EA. Gastrointestinal and Liver Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier; 2005: 608-611.
Rosai, J. Rosai and Ackerman's Surgical Pathology. 9th Ed. Philadelphia, PA: Elsevier; 2004: 1006-8.