
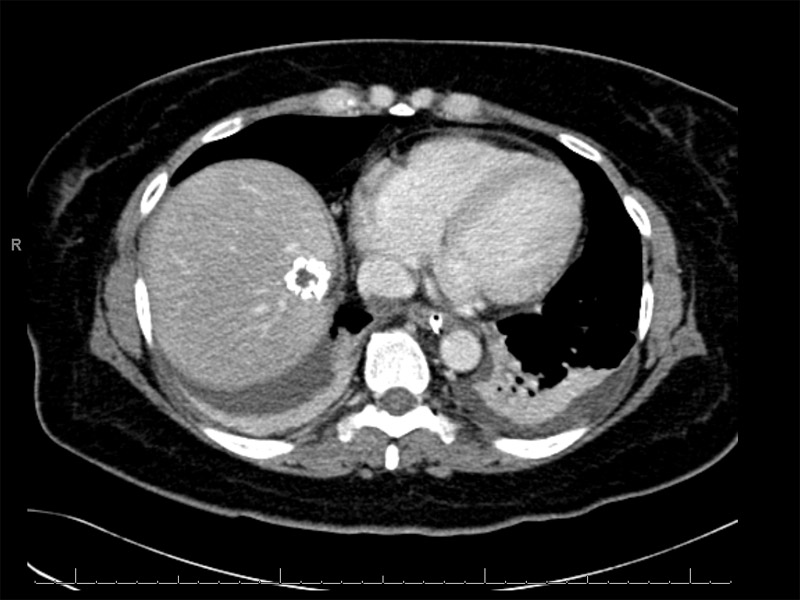
There is a focal well defined hepatic lesion in the periphery of the right lobe of the liver near the dome. It has peripheral coarse calcification and centrally has low attenuation relative to hepatic parenchyma on contrasted imaging. The findings are nonspecific. The pattern of calcification is associated with usually benign or indolent processes, particularly granulomatous disease, however the ddx includes angiomatous tumors and calcifying (including treated) metastases. Most tumors with this specific histology are not so heavily calcified
){kind=link}
FNA shows mildly atypical polygonal cells, singly dispersed. The chromatin is fine and nucleoli are occasionally prominent, as in this case. Cytology findings are fairly nonspecific and must be correlated with the core biopsy. Binucleation may be seen.
){kind=link}
FNA of the lesion also demonstrates these vacuolated blister cells. These mimic signet rings cells, but do not contain mucin.
){kind=link}
Infiltration of the hepatic parenchyma by small cords of an epithelioid cell population. Some cells contain intracytoplasmic lumens (so-called blister cells) which may occasionally contain red blood cells.
){kind=link}
The stroma can be myxoid and sclerotic, as seen here. Necrosis and collagenous necrobiosis may be seen.
){kind=link}
The epithelioid malignant cells can protrude into vascular lumens. Note the polypoid tufting (top, left of center) of the cells. Atypia is present but it is never severe.
){kind=link}
Alcian blue emphasizes the myxohyaline stroma.
){kind=link}
CD31 highlights the membranes of the neoplastic endothelial cells. It is probably the best marker, at least weakly positive in most of these tumors. CD34 is slightly less sensitive but also positive in the vast majority.
){kind=link}
D2-40 highlights the endothelial cells. D2-40, a relatively new IHC marker that highlights lymphatic endothelial cells, has been used in a variety of lymphovascular lesions including lymphangioma, Kaposi sarcoma, and hemangioendothelioma (Kalof).
){kind=link}
Keratin 7 highlights the neoplastic endothelial cells. Keratin 18 is also frequently expressed.
){kind=link}
Keratin AE1/AE3 also stains the tumor cells in this case. Approximately 15% of EHE stain positively with this cytokeratin (Iacobuzio).
){kind=link}
Epithelioid hemangioendothelioma is a low grade malignant vascular neoplasm that have been described in the soft tissues, lung, liver and other sites. It lies between benign hemangioma and angiosarcoma in terms of its behavior. Its course can be unpredictable with patients surviving only a few months to many years after diagnosis.
Grossly, the lesions are nodular with an ill-defined border. In later stages, the nodules may coalesce. The tumor may be multifocal and involve both lobes of the liver. The cut surfaces are gray-white and may be gritty (calcifications). Unlike angiosarcoma, vascular blood-filled spaces are not prominent (Fletcher).
Histologically, the lesion is paucicellular in the center with more proliferative areas in the periphery. Neoplastic endothelial cells with either an epithelioid or dendritic morphology proliferative between the sinusoids. The stroma may be myxoid, sclerotic and occasionally calcified. The presence of the "blister cell", endothelial cells that contain intracytoplasmic lumina, is a characteristic feature. Occasionally, red blood cells can be seen within these small lumens.
Compared to epithelioid hemangioendothelioma, angiosarcoma exhibits more atypia, mitotic activity and necrosis. The entrapped bile ducts and fibrotic appearance may simulate areas seen in cholangiocarcinoma.
EHE can arise in any age group except for children, and most commonly affects middle-aged adults with a female predilection. There is a purported association with oral contraceptive use, but this association is not well substantiated. They typically involve deep and superficial soft tissues of the extremities, and may originate in the vein. The lung may also be a primary site. When involving the liver, patients present with abdominal pain and weight loss. Severe complications may include hepatic rupture, Budd-Chiari syndrome, portal hypertension (as a result of hepatic venous outflow obstruction) and liver failure.
Treatment ranges from chemotherapy and radiation, to resection. For those in the liver, iver transplantation at an early stage greatly improves the prognosis.
Overall, these behave in a somewhat unpredictable manner. In followup of 60 case, the median survival was 77 months (Makhlouf). Thus, although prognosis is more favorable compared to angiosarcoma (mean survival of 6 months), EHE can still be a very aggressive tumor.
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 440-1.
Iacobuzio-Donahue CA, Montgomery EA. Gastrointestinal and Liver Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier; 2005: 619-22.
Kalof AN, Cooper K. D2-40 immunohistochemistry--so far! Adv Anat Pathol. 2009 Jan;16(1):62-4.
Makhlouf HR, Ishak KG, Goodman ZD. Epithelioid hemangioendothelioma of the liver: a clinicopathologic study of 137 cases. Cancer. 1999 Feb 1;85(3):562-82.
Rosai, J. Rosai and Ackerman's Surgical Pathology. 9th Ed. Philadelphia, PA: Elsevier; 2004: 1009.